2025 Inequality Landscape
Foreword
Executive Summary
Introduction
Part 1: Progress on key trends
Progress on key trends
As was the case in SHERU’s 2024 Inequality Landscape, we start with two high level indicators that give a snapshot of health and socio-economic outcomes: life expectancy and median income. Both indicators show a similar small improvement in the latest data, seemingly recovering slightly from a pandemic related downturn in the preceding years.
Figure 1.1 Life expectancy at birth, in years
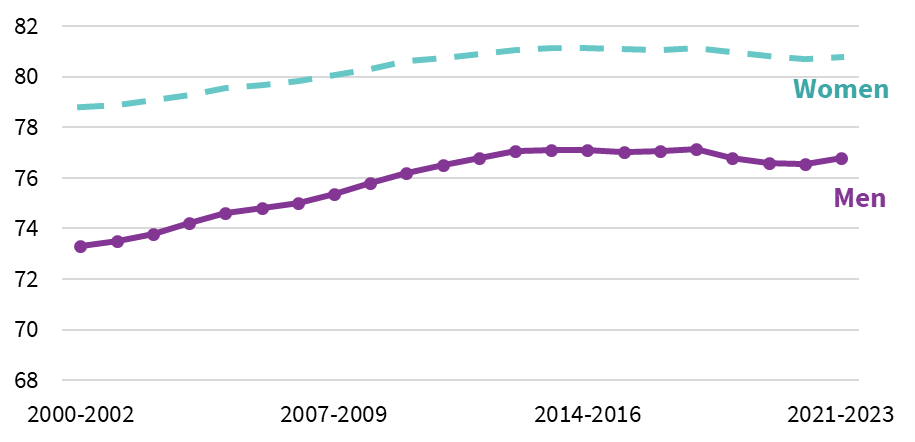
Source: National Records of Scotland, 2024 (9)
Figure 1.2 Median weekly household incomes (in 2023-24 prices) before housing costs
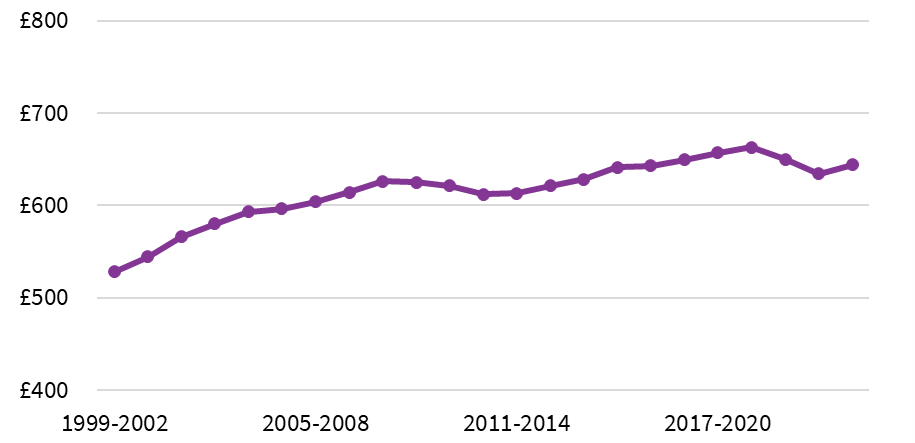
Source: Scottish Government, 2025 (10)
Pre-pandemic, there was evidence of a flattening of the long-run trend of improvement in life expectancy.
Mirroring life expectancy, the long-term rise in median income flattened after the 2008 financial crisis and during the 2010s, a period marked by UK Government austerity policies that reduced public spending. It is widely accepted that this austerity period through the 2010s contributed to the subsequent decline in life expectancy and left public services in a fragile state going into the pandemic (2). Ongoing fiscal restrictions on public spending have made public service recovery challenging, especially in the face of increasing demands (11,12). The ongoing fragility of many public services in Scotland remains a stark challenge for efforts to reduce health inequalities.
Several studies published in 2024 and 2025 have added to the growing evidence base suggesting that the scale of life expectancy declines during the pandemic was linked to the pre-pandemic slowdown in life expectancy improvements (13–15). Examining trends across European countries, a Global Burden of Diseases, Injuries and Risk Factors study found that nations that had made the most progress in improving population health pre-Covid were able to maintain those improvements through the pandemic (14). Sweden, Norway and Ireland even recorded improvements in mortality rates between 2019 and 2021, with improvements in mortality rates for non-Covid conditions outweighing the impact of deaths related to respiratory causes. By contrast, countries that had seen more limited reductions in mortality, particularly from cardiovascular disease and cancers, between 2011 and 2019 experienced little or no progress in reducing deaths from non-Covid causes between 2019-2021. Scotland and Greece were singled out as the worst performing in this regard with no notable reductions in mortality from non-Covid causes over the period. The impact of austerity was given as a possible cause of the relatively poor performance of the UK nations, Greece and Italy on broader mortality rates in the run-up to and during the pandemic.
New analysis released in the last year also includes a systematic review across high-income countries (16) and a book by Glasgow based academics David Walsh and Gerry McCartney that provides an in-depth assessment of UK experiences compared to other high-income countries (15). Both conclude that austerity led to negative health outcomes and that the UK was particularly negatively affected. Walsh and Macartney’s book attributes this to the fact austerity policies in the UK disproportionally impacted the most vulnerable populations, including those on low incomes. Their analysis identifies mental health as a key pathway connecting austerity policies to poor health outcomes. This aligns with earlier work published by VOX, a national mental health service user led organisation based within Scotland, which cites multiple examples of people describing how cuts to public services during the austerity years exacerbated their mental health challenges. For example:
“I’ve gone from someone who lived/worked full time despite an underlying mental health condition, to someone unable to work, unable to access health care (refused) or community support (When I have tried I’m told I am too unwell and need health care first) reliant on social care. The social care I’m allocated is unable to meet my needs. The Service I have found helpful is closing due to council cuts. I can’t see any hope at all; I’ve tried to keep going despite deteriorating health, but the removal of hope by both health care, social care cuts, benefit freezes leave me just functioning in survival mode and [I am] looking forward to the morning when I don’t wake up and don’t have to suffer anymore.”
VOX, 2017 (17)
A couple of recent studies provide further evidence of the mechanisms and pathways linking austerity to poorer health outcomes, placing a similarly strong emphasis on mental health. Mason et al. (2024) found that housing payment difficulties, worsened by austerity, raised the risk of mental health disorders and sleep disturbances, especially among renters, young people, and low-income families (18). While Taylor et al. (2024) linked increased foodbank use to welfare cuts, sanctions, and benefit delays, with users reporting worsened mental and physical health due to stress, stigma, and poor nutrition (19). For further evidence of the links between austerity and health outcomes, see SHERU’s June 2025 Spotlight on Research: Exploring the Health Impacts of Austerity (20).
High Level Indicators of Health Inequality
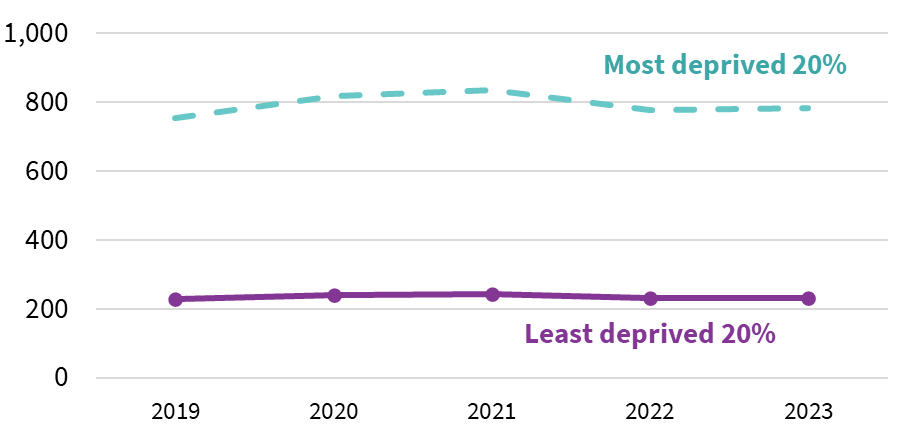
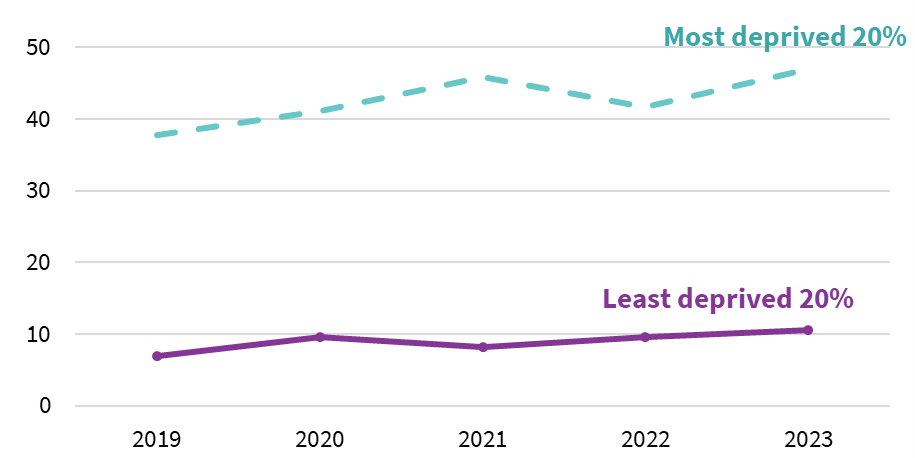
Delays in the publishing of indicators on deaths related to alcohol mean we cannot provide an update on all indicators included in our 2024 report. However, we do have new data on a number of indicators, including early mortality. This shows that, after a narrowing of the early mortality gap between most and least deprived areas in 2022, there was no change in 2023 (Figure 1.3).
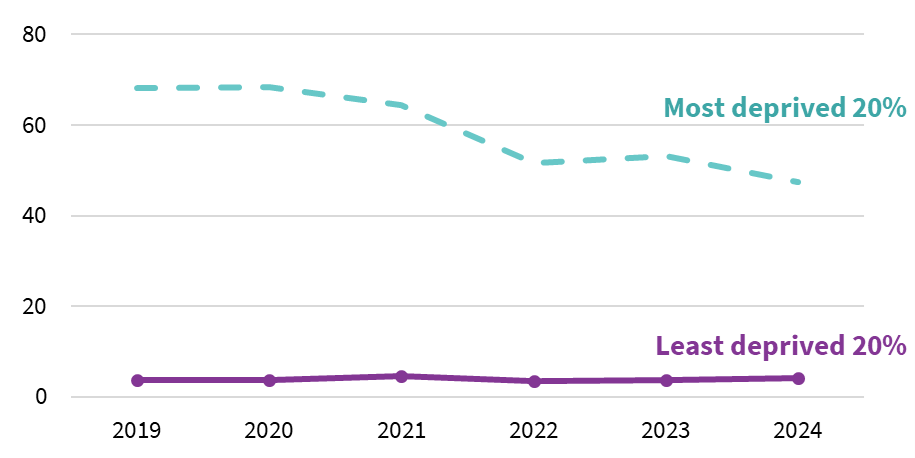
If we compare the most and least deprived areas of Scotland, the most recent (2023) data shows that there has been a slight narrowing of the gap in deaths from coronary heart disease and cancer (the most common causes of death in Scotland) (Figure 1.4) (21).
For cancer, the improvement is unfortunately due to an increase in mortality rates in the least deprived areas. In contrast, for CHD, it reflects a reduction in mortality rates in the most deprived areas, with no change in the least deprived.
Reviews of international evidence, and new comparative research, find that risk factors for cancer and cardiovascular disease tend to be higher in lower-income groups and in groups with less education (14,22,23). Common risk factors for cancer and heart disease include smoking, low levels of physical activity, alcohol consumption, poor diet, and being overweight and obesity. Several countries, including Scotland, have managed to reduce some of these risk factors at population level in recent decades but large inequalities remain (24).
Figure 1.3 Early mortality rate (under 75) (age-sex standardised rate per 100,000 population)
Source: National Records of Scotland (2024) (25)
Figure 1.4 Difference in mortality rates for cancer and coronary heart disease (CHD) (age-sex standardised rate per 100,000) between the 20% most and least deprived areas of Scotland

Source: National Records of Scotland (2024) (25)
Research suggests that policy measures that are mandatory and population wide (such as product reformulation, fiscal measures and restrictions on products and marketing) are both more effective in achieving reductions in risk factors at population level, and more likely to reduce inequalities, than voluntary measures (such as health promotion campaigns) (26,27). The multifaceted tobacco control measures implemented in Scotland and the wider UK in the 2000s have yet to be mirrored for alcohol and unhealthy food. Indeed, Scotland’s post-devolution food reformulation and public education efforts have been primarily voluntary, with limited impact on increasing fruit and vegetable consumption to recommended levels (14). The underlying material, social and environmental factors associated with disadvantage have been identified as a significant barrier to the effectiveness of interventions designed to reduce key risk factors (28).
Figure 1.5 Drug-related mortality rate (age-sex standardised rate per 100,000)
Source: National Records of Scotland (2025) (29)
Figure 1.6 Alcohol specific mortality rate (age-sex standardised rate per 100,000)
Source: National Records of Scotland (2024) (29)
Poverty and household income
Household income plays a critical role in explaining health inequalities, and there are dramatic differences in health outcomes between wealthy and poor groups. Limited income makes it harder for people to adopt healthy behaviours and creates stress for households struggling to make ends meet. There are obvious negative outcomes from this: people may struggle to afford essentials like food or heating. Perhaps less obviously, the gap between those with low incomes and those with middle or higher incomes can also lead to social isolation – a factor that negatively impacts health (30). This can be because people cannot afford to participate in common societal activities, such as paid-for school trips or social events that involve paying for food or drink but can also be a result of people trying to avoid the stigma of poverty (31).
The latest data incorporates the financial year 2023-24 where the “cost of living” crisis was at its height. These data are presented as real-terms changes (all previous year’s figures are uprated to the latest year) so the uptick for most households is a real improvement in living standards. Factors which will have impacted on incomes in this year include pay rises (including the National Living Wage and the Minimum Wage) and additional targeted cost of living payments.
Median incomes, illustrated in Figure 2.1, rose in the three-year period[1] from 2021 to 2024 relative to the previous three-year period (2020-2023) across most population groups, with the exception of pensioners which may be at least partly explained by their greater reliance on fixed incomes and savings which tend not to adjust in line with inflation unlike earnings from employment.
The most recent data, illustrated in Figure 2.2, show that poverty has reduced slightly, indicating a relative improvement in living standards for those at the bottom of the income distribution. This has particularly been the case for children (see page 17, Better news on child poverty).
In last year’s report, we noted a particularly concerning trend for poverty among 16–24-year-olds, a period when many people are leaving home and transitioning to financial independence. Promisingly, there is now evidence that poverty is also starting to reduce for this age group although, as Figure 2.3 shows, rates remain far above the Scottish average.
Figure 2.1 Median weekly equivalised household incomes (in 2023-24 prices) before housing costs
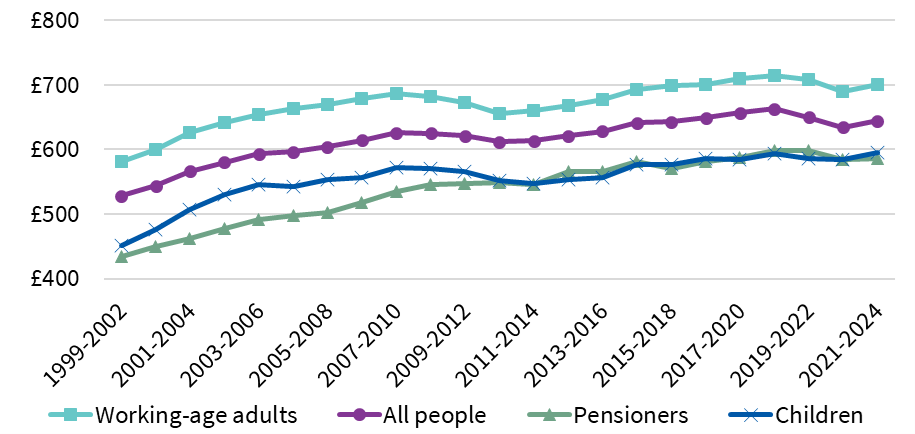
Source: Scottish Government (2025) (32)
Figure 2.2 Average yearly proportion of the Scottish population in relative and absolute poverty (after housing costs)
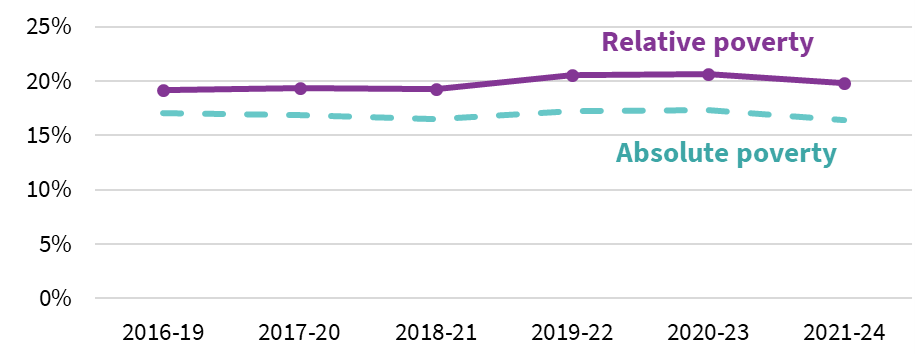
Source: Scottish Government (2025) (32)
Figure 2.3 Average yearly proportion of non-dependent 16- 24-year-olds in relative poverty (after housing costs)
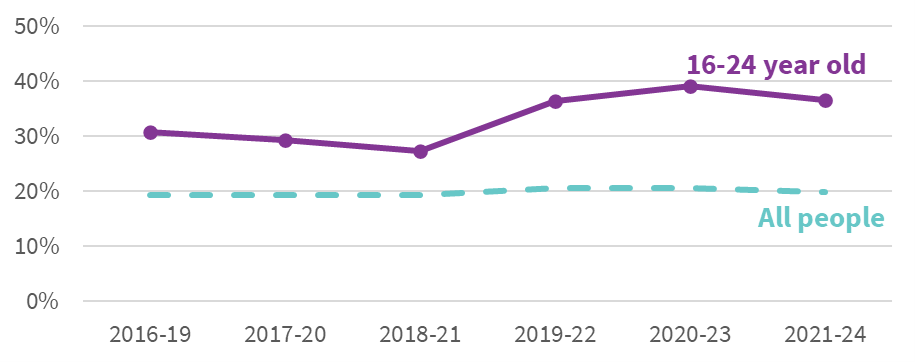
Source: Scottish Government (2025) (32)
A 2025 review of children and young people’s experiences of poverty in Scotland provides additional evidence of the stress that experiencing poverty causes for this age group:
“It’s not healthy to have to regulate when you receive heat or not nor having to buy less/ worst quality food.”
16, Dundee (33)
“You can’t even sleep – worrying about not having food to eat. They [Council] need to provide food for young people.”
Unaccompanied, asylum-seeking young person (33)
Qualitative accounts also identify some place-based variations in young people’s experiences (e.g., between rural and urban areas):
“I get £67 per week. When I lived in Inverness this was enough to buy all my food. Now I live in [village] it is more difficult because they don’t have Lidl or Aldi, only a Co-op which is more expensive.”
Participant (33)
Analysis for households which contain one or more people from a minority ethnic group show that rates have also begun to improve for Asian/Asian British Households, although rates remain far above groups described as “White – Other” or “White – British”. The rate for “White – Other” has now moved closer in line with “White – British” whereas the combined rates for mixed ethnic groups, Black or Black British, and Other ethnicities have remained static (Figure 2.4).
Figure 2.4 Average yearly proportion of households including a member from an ethnic minority background in relative poverty (after housing costs)
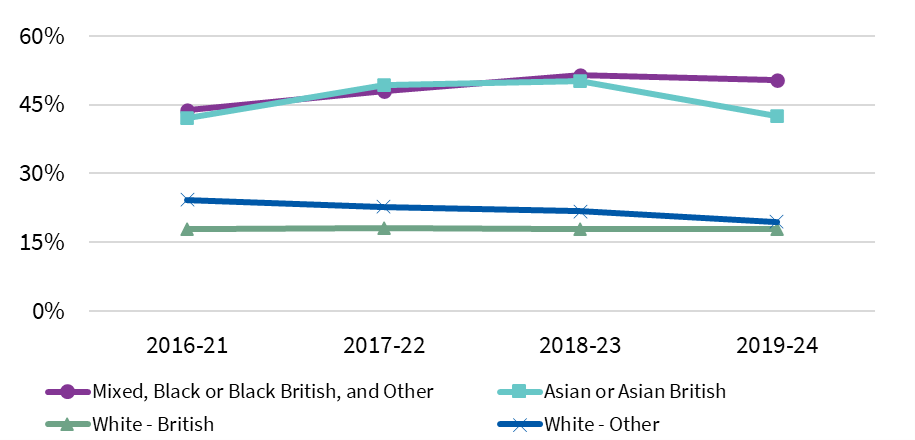
Source: Scottish Government (2025) (32)
Newly published research exploring the health and wellbeing experiences of minority ethnic unpaid carers in Scotland suggests that eligibility restrictions and challenges negotiating an unfamiliar social security system may both contribute to poverty in Scotland’s ethnic minority communities:
“I was alone, I didn’t have children. But then when you’re an immigrant you don’t have access, no recourse to public funds, what it means is you are always existing on eggshells… you’re just day to day. It’s a very, very stressful existence.”
Female, 45-64, Pakistani (34)
“The only reason I got the allowance was that Al-Masaar [a charity for minority ethnic carers in Forth Valley – now renamed Coalition of Carers and Rise Forth Valley] helped me complete the forms. If that wouldn’t have happened, then I still wouldn’t be getting that allowance and I’m not sure how I’d cope.”
Female, 45-64, African (34)
Better news on child poverty
One of the most significant policy responses to tackling poverty in recent years has been the Scottish Child Payment. As of April 2025, this provides an additional £27.15 per child, per week, to all eligible families (up from £26.50 in 2024-25). Data from March 2025 suggest approximately 326,000 children were benefiting from the payment, which equates to around a third of all children in Scotland (35).
Our report last year highlighted concerns that the increase in the Scottish Child Payment was not feeding through to income and poverty data as expected. We noted that this was likely to relate to issues with data collection.
Since last year, there has been a welcome change in the methodology for capturing the Scottish Child Payment. As Figure 2.5 shows, data released in March 2025 (for the year 2023-24) demonstrate a small decline in child poverty and indications of a deviation from the UK trend. Whilst the change is small when looking at the three-year average, we would expect this trend to be consolidated as more years of data is gathered.
Figure 2.5 Average proportion of children in Scotland and the UK in relative poverty (after housing costs)
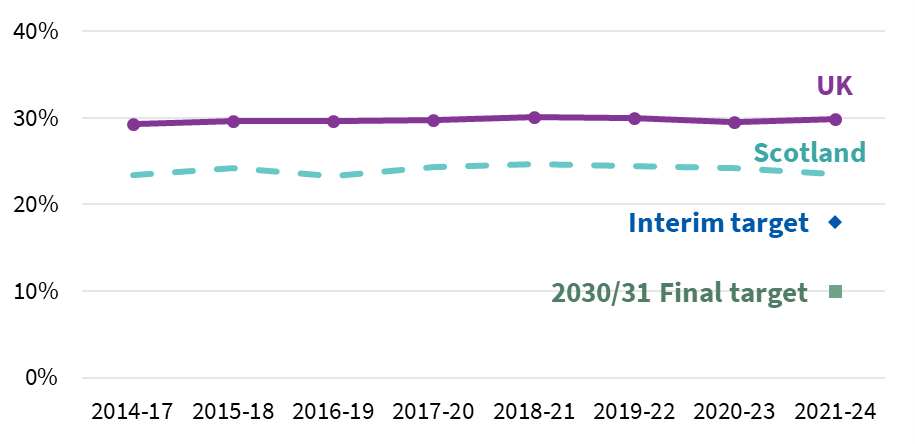
Source: Scottish Government (2025) (32)
Note: Data collected for the financial year 2020/21 is not included due to issues with data quality in this year.
Following discussions with Scottish Government, colleagues from the Fraser of Allander Institute tested the new methodology to assess whether it did a better job of capturing children who were eligible for the payment. Ultimately, they concluded that adopting the new methodology sooner would not have changed the poverty rate in the 2022-23 data, but the new method does a much better job of capturing the number of people receiving SCP, giving us more confidence in figures going forward (36).
In our 2024 Inequality Landscape report we said that, even if the Scottish Child Payment was showing up in the data as expected, Scotland would still be some distance away from meeting its statutory child poverty targets (1). Unfortunately, the new data released in March 2025 confirmed that the 2023-24 interim child poverty target was not met.
SHERU analysis, published shortly after the new data release, also looked at child poverty for different social groups (37). This showed that child poverty was falling for lone parents, and children living in a household where at least one person was from a minority ethnic group but was increasing for families with three or more children (Figure 2.6) and had plateaued for households with at least one disabled person. And while child poverty fell in urban areas, it rose in rural areas. This shows that, although the Scottish Child Payment appears to be reducing child poverty overall, there are other countervailing factors that may be limiting its impact on some families.
Figure 2.6 Proportion of households in relative poverty by number of children in household
Source: Scottish Government (2025) (32)
While the Scottish Child Payment at its current rate will not be a sufficient policy intervention to meet child poverty targets, the value of these payments to families has continued to be articulated by those who receive the payment. For example, a participant in the Changing Realities project shared the following account of the difference the payment was making with the First Minister in April 2025:
“Now, with the payment at £26.70 per week, it has allowed me and my son to afford social and educational activities we would otherwise miss. It has reduced financial pressure, supported my son’s health, and given us more breathing space to enjoy life. Kids need to thrive – not just survive. The Scottish Child Payment has been instrumental in our lives. It has enabled me to invest in healthier food, which supports my son’s learning and brings me peace of mind. […] As someone with lived experience of mental health challenges, the SCP has been vital in easing stress and improving our quality of life. This has had a direct, positive impact on my son… […] While I applaud the government’s commitment to tackling this through the SCP, more is needed.”
Isabella-rose F (38)
This extract reflects broader, lived experience accounts, with families generally reporting that the payment helps them to cover essential costs and access activities for their children, but remains insufficient to fully alleviate the anxiety associated with economic insecurity (39). A recent Scottish Government report, Learning from 25 Years of Prevention, includes the Scottish Child Payment as a case study of primary prevention, though acknowledges the evidence of impacts is still emerging (40). In September 2025, the Scottish Government published a report offering new insights into claimants’ accounts of the Scottish Child Payment’s impact, though further work is required to more robustly assess the effects on health outcomes (41).
The year ahead will bring some significant changes to how data on income and poverty is captured across the UK. DWP will be linking their administrative data on benefit income and potentially HMRC data on earnings. The current source of data, which we have relied on in this section, comes from the Households Below Average Income Survey, which significantly underreports income from benefits. This administrative data linking will ease this issue and, as such, we expect households accessing benefits to see increases in their income in the official data which means, holding all else equal, we should see a decline in poverty rates.
As yet, the extent to which devolved Scottish benefits will be included in this administrative data linkage is unknown. Without such inclusion (or some new methodological innovations, as has now happened for the Scottish Child Payment), incomes for people in Scotland who draw on Social Security Scotland administered disability and carer benefits will start to look markedly (and misleadingly) worse compared to people in England and Wales who draw on DWP administered benefits.
Beyond these data innovation related changes, there is likely to be little change in income and poverty with no new policies likely to positively impact poverty rates having been introduced in the UK or Scotland in 2024-25. The withdrawal of some cost-of-living payments that were paid during the financial year 2023-24 could show up as a reduction in incomes for some households.
While efforts to mitigate the impact of the two-child benefit limit in Scotland should show in future data, this will likely not be before 2026-27. Countering this, the impact of UK Government welfare reforms, for example the reduction in the health-related top ups to UC for new claimants, will also start to take effect in 2026-27.
Spotlight on debt
Debt is an important aspect of the money available for household spending which is not captured in most data on income and poverty. It can take on many forms but is generally considered to be money that individuals or households are legally obligated to repay in future. Debt may accrue for a wide range of reasons, often relating to household needs, and can accrue on a short-term or long-term basis.
Debt is not always harmful if repayments are manageable. Mortgages, for example, spread the cost of an asset and can raise living standards. Problems arise when debt becomes unaffordable (“over-indebtedness”), which is linked to poorer physical and mental health and is both a cause and a consequence of poverty (42).
Levels of debt are usually captured in surveys that look at household assets (in Scotland, the main data source is the Wealth and Assets Survey, which is conducted every two years, although along with other statistical publications in the UK at present, there are concerns over robustness of the latest data). Surveys typically rely on people’s willingness to declare debt. Stigma, especially around some debts, such as gambling, can lead to under-reporting (43).
The ongoing issues around the rising cost of living continue to exert significant financial pressure on households across Scotland and for some people this has compromised their ability to manage and service existing debts. Inequalities in available financial services and support mean that low-income households are often forced to take on high interest loans, further exacerbating income pressures (42).
“We’ve had no savings, since the beginning of COVID. Everything has gone up – our overdraft is maxed out most of the time. The safety net is being used. We can plan for things and save up but when a big-ticket item goes, the money isn’t there. When the cooker went – we applied for a loan, got knocked back. I had to ask my dad to put it on his credit card and pay him back. We didn’t have a choice – we needed to feed the kids. The same bank won’t give us a loan to repay at £20 a month, but they’ll happily take £17 a month in overdraft charges”.
Gordon (44)
Public debt (i.e., debt which is monies owed to public bodies e.g. local authorities such as rent arrears, council tax arrears, school meal debt or DWP repayment of Universal Credit advances) also continues to be a problem faced by low-income households in Scotland. Analysis collated on the Universal Credit in Scotland has found that, in February 2025 alone, £17.4 million is being deducted from Universal Credit payments across Scotland. When annualised, this amounts to nearly £210 million in deductions each year (45).
In 2025, Citizens Advice Scotland noted that council tax debt was the single most common debt type people had been seeking advice about (46). An earlier Citizens Advice Scotland report expressed concern that councils have been sharply increasing debt enforcement (in contrast to other types of creditors), using tools such as bank account freezes, wage and benefit deductions, and “Exceptional Attachments” that let officers enter homes to seize goods (47).
Research in Scotland has found that household debt is disproportionally impacting families with lone parents with a disabled child or children in the house (45). Qualitative research on the experience of households affected by public debt in Scotland found that this was exacerbating household income inadequacy, leaving some people taking on other forms of consumer debt to cope:
“So I was paying all this stuff out and I literally was struggling. It was making my mental health worse. Obviously, I had a lot to deal with already and it was horrible. So that was like – I ended up getting in debt with my housing benefit as well. So then I got into rent arrears because I didn’t pay that into my rent because I physically, I had two children I physically couldn’t do it”
Laura (48)
Policymakers have acknowledged this issue in Scotland, and we have seen, for example, investment to support local authorities in writing off school meal debt to help mitigate the cost-of-living crisis (49). In the coming year, SHERU will work with others to better understand the role that household debt is playing in Scotland as a socio-economic determinant of health inequalities and the potential for policy measures to help reduce these impacts
[1] As is standard practice, we use three-year averages to illustrate trends in incomes and poverty. However, because of data issues in 2020-21, any period that would normally include that year has instead been calculated using a two-year average.
Education & early years
The relationship between education and health is complex. Education is shaped by the same socio-economic conditions that influence health and is sometimes used as a proxy for childhood socio-economic position (50). Many health outcomes are worse among people with less education, but evidence that more education directly improves adult health is mixed. There is evidence that educational attainment mediates links between childhood socio-economic adversity and health-harming behaviours in adulthood (50) and that bullying in childhood is a risk factor for a wide range of poor social, health, and economic outcomes in adulthood (51). We also know that experiences at school can provide the foundation for secure living standards in adulthood (52), through qualifications achieved, wider skills and capacities, and via social networks that are enabled (53).
Inequalities begin before birth (54). The importance of the early years for health across the life course is well established, with broad consensus on the need for early support and interventions to reduce health inequalities (55,56). Scottish policy aims to reduce their impact by supporting families – financially and through early-years and school settings. Despite sustained efforts to reduce the attainment gap, such as implementing policy initiatives including Getting it Right for Every Child (57) and The Promise (58), indicators of childhood inequality remain stubbornly high.
Lower socio-economic circumstances affect many aspects of early family life. Across high-income countries, people living in deprived circumstances experience worse pregnancy outcomes (59). In Scotland, childhood experiences are shaped by limited household income, which reduces the potential to participate in social activities; family stress, which arises from difficulties meeting essential costs including food, housing, energy; and the condition and quality of accommodation and key services (notably education). These socio-economic and contextual factors interact to influence child development, wellbeing and families’ long-term opportunities.
Play – at home and in the community – is critical in early childhood. Its importance is recognised in Article 31 (Leisure, play and culture) of the UN Convention on the Rights of the Child (1990) (60). Play underpins children’s language, physical and cognitive development and other contributors to health and wellbeing (61). Yet many low-income families in Scotland report barriers to high-quality play, including prohibitive costs and a lack of suitable, accessible spaces (62).
“Why do you have to be minted to take your baby swimming?”
Parent in Scotland (63)
“There is nowhere in my street that is safe to meet up with friends and play, my friends live 10/15 min walk from me, my mum won’t let me out by myself because the traffic is busy and it’s boring by myself if my friends aren’t with me.”
Boy, 9, Glasgow (61)
Early years have been a core policy focus in Scotland, with investment in flagship measures such as funded childcare for eligible two-year-olds and 1,140 hours of free childcare for three- and four-year-olds through funded early education and childcare (ELC) providers (64). This reflects policy recognition that “a fully functioning childcare sector is a pivotal part of Scotland’s national economic infrastructure” (65). Despite this progress, gaps remain in the cost and availability of provision. A Joseph Rowntree Foundation poll of parents with children under age five found that nine in 10 parents wanted more funded early years childcare. The research also identified groups facing additional barriers, including families in part-time, insecure employment and households with irregular or shift work (66).
Wider research supports these findings. A longitudinal study tracking workers in Scotland’s hospitality sector – typically characterised by low pay and insecure hours – reported similar challenges, with parents struggling to access childcare that fits their work patterns.
“Because me and my husband, we both work extra hours every week to be afford – like to be able to afford to live kind of thing. Without the extra hours, we wouldn’t be able to survive”
Carla, remote rural area (67)
Free childcare is an important policy, but it must be integrated with other services to work well for families.
“I began a college course… I had to leave home at 7am to walk across town with my child to childminder, as no buses to that area, then walk back across town to catch bus then run, on foot, to college for a 9am start…. I had a breakdown as both myself and my child were exhausted from this due to heavy traffic and late picking up child and being charged late fees.”
Single parent, one child, rural area (68)
The early years are a critical period for physical, cognitive and socio-emotional development, with long-term effects on health and life chances. Targeted support at this stage can reduce inequalities and build a stronger foundation for future learning and there is a clear need to focus on aligning provision to the needs of low-income families. As such, educational attainment is closely linked to early experiences and to the availability of sustained support throughout a child’s learning journey.
Improving children’s lives and attainment depends on cross-government policy, including efforts to reduce child poverty and improve housing, both of which have been the subject of high-level Scottish Government strategies. These actions should improve outcomes, but this is dependent on effective implementation. Monitoring and evaluation are needed to track their impact on both immediate outcomes and more distal health experiences.
The gap in developmental concerns at 27-30 months narrowed slightly over the last year but remains wide at 15.6 percentage points – close to the highest level since 2014/15. In the most deprived areas, levels are similar to those seen nearly a decade ago, suggesting persistent early development challenges with little long-term improvement (Figure 3.1).
Figure 3.1 Proportion of children who have developmental concerns at 27-30 months
Source: Public Health Scotland (2025) (69)
The latest data on inequalities in educational outcomes at primary school level shows little change on last year, meaning the gaps in meeting grade-level expectations between the most and least deprived pupils remain similar to those seen before the pandemic (Figure 3.2).
Figure 3.2 Proportion of P1 and P7 students meeting grade level expectations in reading
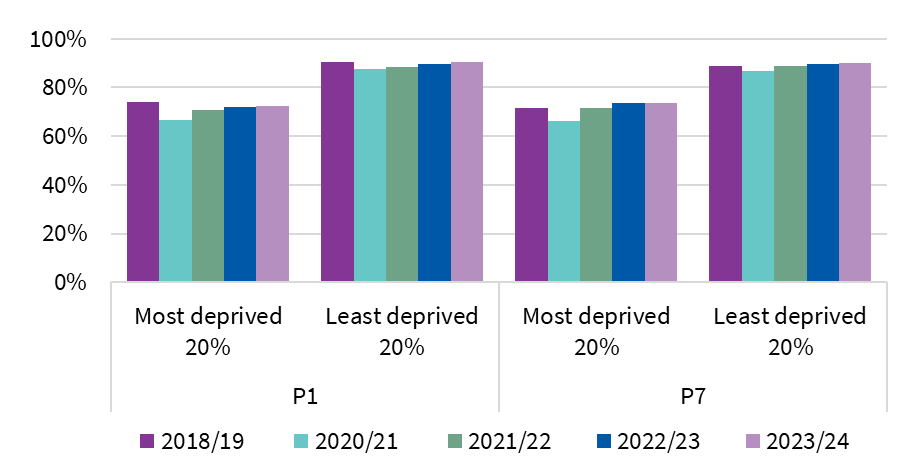
Source: Scottish Government (2024) (70)
Rates of attendance at school have been falling in recent years, across all pupils. Moreover, pupils from the most deprived areas continue to experience lower attendance rates compared to those from the least deprived areas. Sickness absence rates are also higher in more deprived areas (which may be a manifestation of early health inequalities). Rates have changed very little in the latest data. This persistent gap in attendance highlights ongoing challenges facing disadvantaged students and a risk of disengagement, which can lead to poorer educational outcomes and exacerbate existing inequalities (Figure 3.3).
Figure 3.3 Proportion of half days of possible attendance recorded as absent in school by students’ deprivation quintile, 2023-24
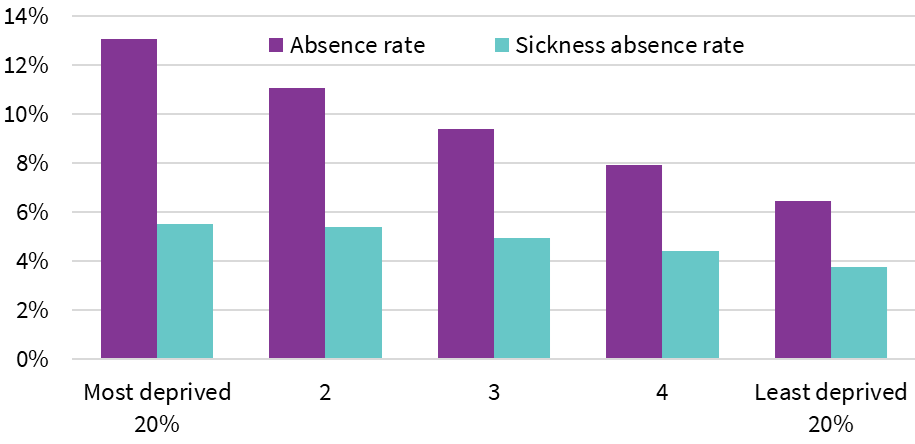
Source: Scottish Government (2025) (71)
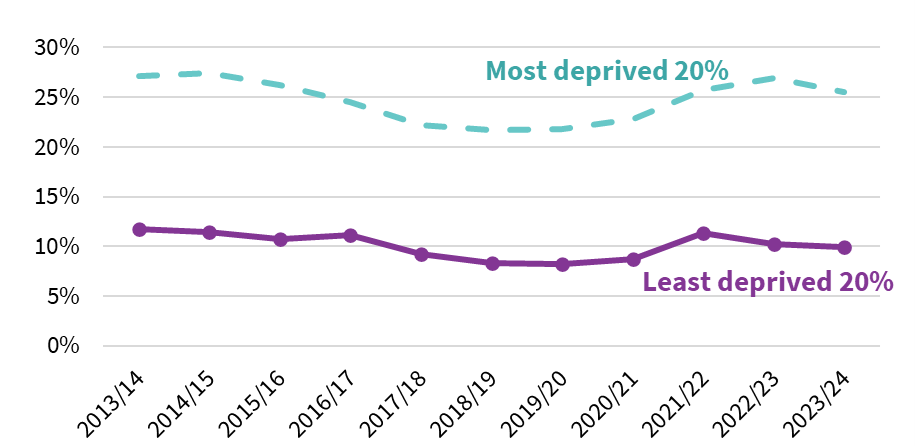
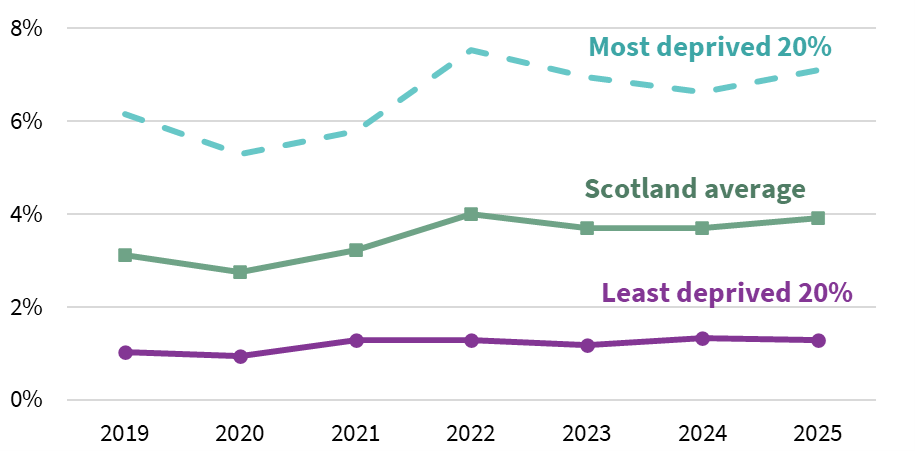
In 2025, Scotland recorded positive progress, with the attainment gap narrowing between the most and least deprived 20% of communities, driven by improved pass rates (grades A-C) across National 5, Higher (Figure 3.4) and Advanced Higher qualification levels. Nonetheless, the rate of improvement remains modest, and the disparity between advantaged and disadvantaged students endures, with the persistent link between poverty and educational outcomes continuing to limit progress.
The Scottish Government’s wider struggle to meet its interim child poverty reduction targets has further hindered efforts, leaving its 2016 commitment to “substantially eliminate” the attainment gap by 2026 increasingly out of reach.
Meanwhile, the gap in higher education participation among 16-19-year-olds remained largely persistent throughout the pandemic, with a modest narrowing in 2024. In 2025, participation rates for the 20% least and most deprived remained largely unchanged, despite a slight widening of the gap compared to the previous year (Figure 3.5).
Figure 3.4 Proportion of candidates attaining grade A-C at Higher
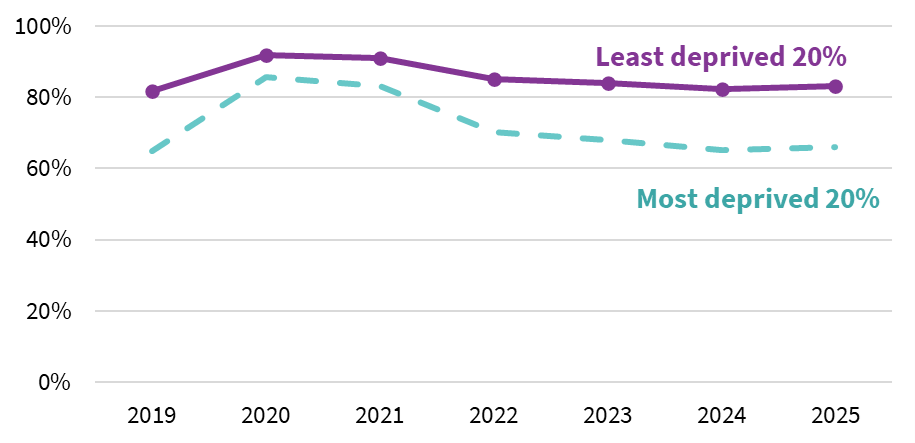
Source: Scottish Qualifications Authority (2025) (72)
Figure 3.5. Proportion of people aged 16-19 participating in higher education
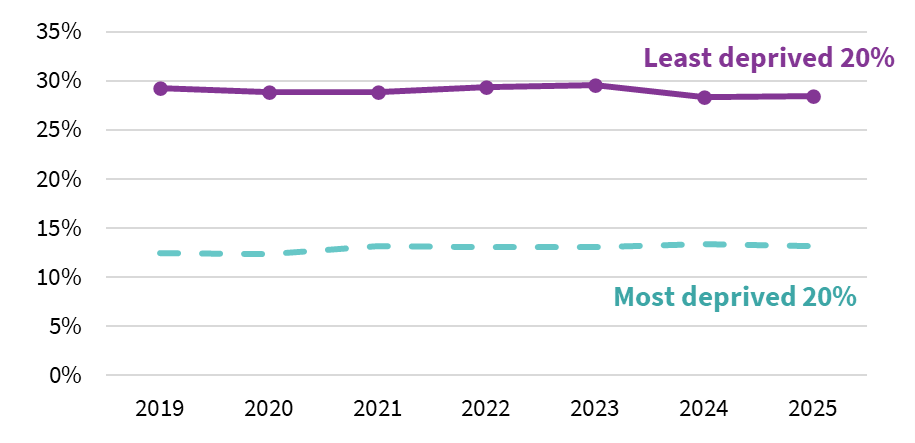
Source: Skills Development Scotland (2025) (73)
A new mixed methods study of Scottish young people from areas of high deprivation who had accessed higher education, features qualitative accounts of their educational journeys. It identifies unequal access to advanced subjects as a key barrier to progress, particularly Advanced Highers, and highlights how this can limit access to some competitive degrees, such as medicine and STEM subjects (74). Many students also felt their educational opportunities had been limited by their schools’ comparative lack of funding and resources, which led to a high staff turnover and limited sense that there were people who cared about their outcomes:
“it’s like vastly different … it’s like actual like teachers and stuff… my school in my last year I did English Higher English and… we had three teachers a week… it’s like the actual lack of like staff and even when you do have staff there’s a lot of staff that are like, ‘aw we’ve given you the resources, if you fail, you fail – I don’t care, go away and learn it’”
Saoirse (74)
Employment
The links between the work that people do and their health are multifaceted. There is a lot of concern about people who are not engaged in the labour market (referred to as economic inactivity), but we also know that quality of work, which encompasses job security, working conditions, and the level of stress associated with a job, plays a critical role in people’s physical and mental health. Both having a job and the quality of that job are linked to earnings, which is a significant component of household income.
Unfortunately, it is becoming increasingly difficult to monitor what is happening with the labour market in Scotland, which means that it is difficult to understand recent trends and the resulting intersection between health and employment. Most data on the labour market in the UK comes from the quarterly Labour Force Survey and the Annual Population Survey, both published by the Office for National Statistics (ONS). The quality of data produced from these sources has come under a lot of scrutiny in the last couple of years due to concerns around falling sample sizes and increasing volatility.
The Scottish Government and the ONS have assessed the reliability of labour market statistics and using their quality thresholds and have found that headline statistics of employment, unemployment and inactivity, are deemed “robust.” However, analysis by the Resolution Foundation for the UK, replicated by SHERU for Scotland, used administrative data from HMRC’s PAYE data, and found evidence to suggest that employment has been stronger than the Labour Force Survey suggests. If this is true, then it follows that the number not in employment (i.e., those categorised as unemployed or economically inactive) may not have risen as much as the LFS suggests (Figure 4.1) (75).
Figure 4.1 Modelled employment rates, 16+
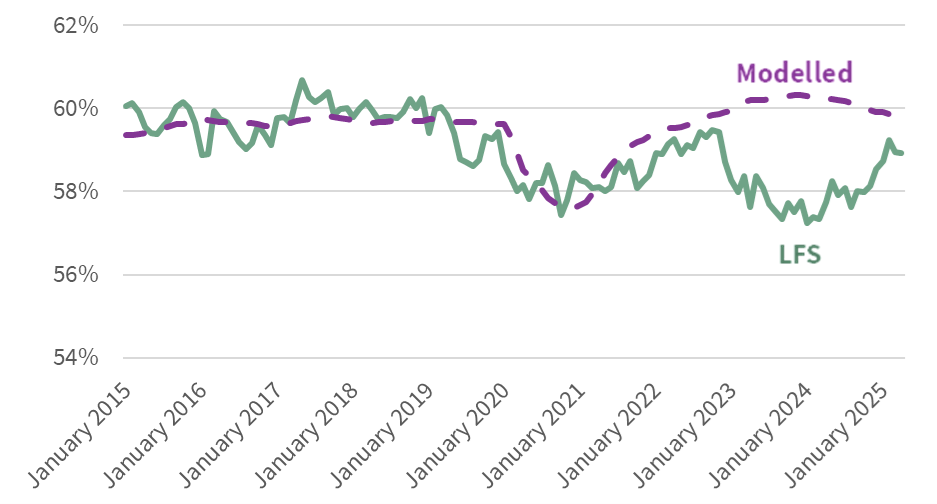
Source: SHERU (75)
For more specific categories with small numbers of responses, there is less confidence from official statisticians in the quality of indicators. For example, the Scottish Government reported lowered confidence in the statistical quality of five out of nine possible survey responses under “reasons for inactivity,” and “whether want to work” in 2023 compared to 2019 (76). Given these issues, we have chosen not to show updated statistics for inactivity by reason in this year’s report. However, the Scottish Government, along with other organisations, continue to use this data widely, perhaps because long-term sickness and student data are rated as “high confidence” in both 2019 and 2023, even though confidence in other reasons for inactivity have declined over time. The current statistics show a rising economic inactivity rate and a large increase shown in the number of people inactive due to long term ill health (77).
Alternative official statistics on inactivity for those aged 16 to 19 exist in Scotland through the Annual Participation Measure. This measure utilises data from Skills Development Scotland’s customer support system. According to these data, the share of 16–19-year-olds confirmed as not participating in employment, education or training rose across Scotland over the past year, reaching 7.1% in the most deprived areas, while remaining stable at 1.3% in the least deprived (Figure 4.2).
Figure 4.2 Proportions of those aged between 16 and 19 who are not participating in education, employment or training
Source: Skills Development Scotland (2025) (73)
Another possible source for insights on the relationship between health and work in Scotland is administrative data from the benefit system. Here there has been an increase in the number of people claiming the health component of Universal Credit (UC) and/or disability benefits. A rise in the number of people on these benefits is not necessarily correlated with an increase in people not working, as people on these benefits may be in work or out of work.
However, we can look at data on the proportion of people on UC who are in work in Scotland. If the increase in people claiming the health component of UC was also correlated with more people being unable to work due to illness or disability, then we would expect to see an increase in the proportion of people on UC who are not in employment.
Figure 4.3 shows, whilst there is evidence of a slight recent rise in the proportion of people accessing on UC who are out of work, the rise is small, and the proportion remains below pre-pandemic levels. We aren’t seeing evidence of step change in the number of people out of work and on UC since the pandemic, but there are other factors that might be affecting this data. For instance, different cohorts across the long-running managed transfer of people from “legacy” benefits such as Employment and Support Allowance may have particular employment characteristics that could skew the data one way or another. Unfortunately, the Department for Work and Pensions (DWP) does not provide a breakdown of employment status for those newly claiming the Health Element of UC.
Figure 4.3 Proportion of those on Universal Credit in Scotland by work status
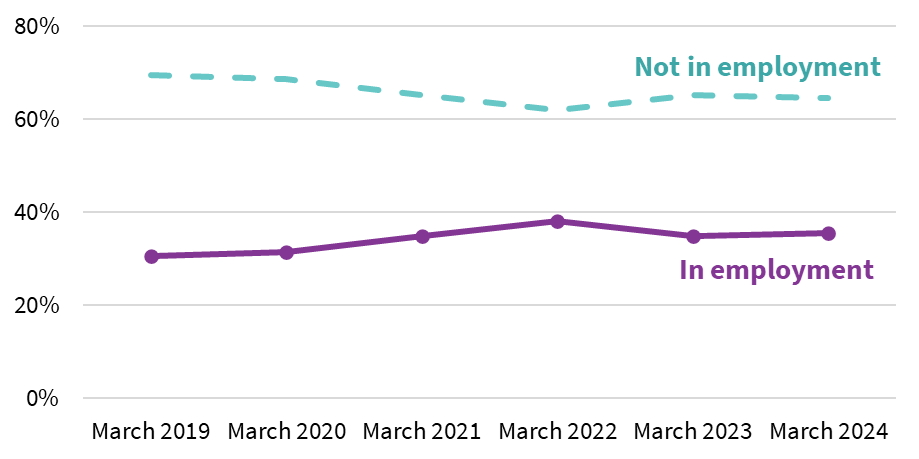
Source: SHERU analysis of DWP (2025) (78)
Social Security Scotland do not publish data on work status for people on devolved disability benefits, but analysis presented by the DWP for PIP for England and Wales in their Get Britain Working green paper showed that, since the pandemic, the proportion of PIP claimants who are employed has started to increase, from 14% in March 2021 to 17% in March 2024 (79). Again, this does not corroborate a trend of rising inactivity due to ill health.
Where does this leave us? Whilst there is evidence from the benefit system and from elsewhere that supports the fact that there are more people seeking additional medical and/or financial help due to ill health (80), there is clearly reasonable doubt that this is leading to the large increase in economic inactivity described by the Labour Force Survey.
We note that a range of high-profile economists have raised concerns on labour market data being used for policy making, including Richard Hughes, chair of the OBR, and the Bank of England Governor, Andrew Bailey. And yet, we see both Scottish Government and UK Government ministers citing Labour Force Survey data uncritically and using this to push ahead with responsive action (81,82). At the UK level, this is part of the discourse justifying controversial welfare reforms, whilst in Scotland, less controversially, these data have been cited in relation to plans to push ahead with a health and work action plan.
“The LFS is essentially useless.”
Xiaowei Xu, senior research economist at the IFS (83)
This is a difficult position for policy makers to be in. If rising economic inactivity related to ill health and disability is real, as the Labour Force Survey suggests, the long-term consequences for both the population and the economy could be severe. And regardless of recent trends, there is a long-standing gap between inactivity rates in Scotland and the rest of the UK due to ill health. Nevertheless, we would like to see appropriate caveats and caution used by the Scottish Government and other public bodies when putting forward labour market evidence to justify policy changes or strategic intent, and more exploration of alternative data sources.
Given the issues with the quantitative data, it is especially important to consider insights from available qualitative research. We have yet to see studies that take a longitudinal approach to understanding employment experiences since the pandemic, but Public Health Scotland published a report in 2025 drawing on participatory research exploring mental health in and out of work (84). The accounts within this report suggest that a lack of flexibility and mental health support within work settings contribute to people feeling unable to stay in work, while a “one size fits all” approach to employment services limits opportunities to return to work for people with ongoing mental health challenges.
“…you must go through occupational health before you start and they knew I have mental health issues but there wasn’t really an offer of ‘Oh, there is such and such a service we provide, and if you feel you need to, you can attend there’. There wasn’t anything like that. Basically, the senior staff were just interested in why I couldn’t do night shift. I was hounded about it.”
Sarah (84)
“[…] it doesn’t work for people’s mental health, a one size fits all rule for people who are looking for work doesn’t work. Because you have got people who are out of work who are way over qualified for jobs that they are forced to apply for just so that the job centre can tick boxes to say that they are applying for jobs and they are wasting time and they can’t actually apply for jobs, like worthwhile jobs, where they would actually be boosting their mental health if they were filling out the applications and they are just sinking down this slippery slope.”
Fiona (84)
One labour market indicator that we can look at with more confidence is earnings. Data on earnings comes from the Annual Survey of Hours and Earnings (ASHE), which is based on a 1% sample of PAYE data and fortunately does not suffer from the same issues that the Labour Force Survey is facing. Here, there has been a marginal narrowing of the gap in the 2024 statistics, driven both by real-terms increases for the bottom 10% (likely partly driven by Minimum Wage and National Living Wage increases) and the median, and real-terms decreases for the top 10%, but the gap remains stubbornly wide (Figure 4.4).
Figure 4.4 Average weekly full-time employment earnings (in 2024 £)
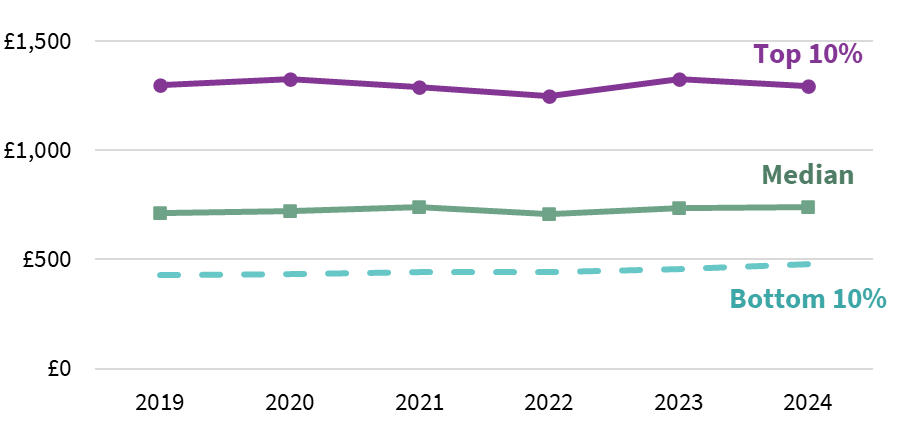
Source: SHERU analysis of the Office for National Statistics (2024) Annual Survey of Hours and Earnings (85)
Housing and homelessness
Housing quality, access, and affordability all shape people’s physical and mental health (86). Housing affordability also affects disposable income, limiting the ability to spend on other necessities. Additionally, insecure housing tenure can be challenging for families seeking stability and, in extreme cases, can lead to homelessness, which is closely related to a wide range of poor health outcomes (87).
Scotland has ambitious aims on new housing, but these are increasingly undermined by the existence of the housing emergency, which is marked by rising homelessness, unaffordable rents, and a slowdown in new builds. This is placing huge pressure on national and local policy responses.
As Figure 5.1 depicts, the latest data on the number of new affordable homes built in Scotland shows a declining trend, particularly for homes built for social rent between 2022-23 and 2024-25. This comes after Scottish Government cuts to the affordable housing budget in 2022-23 and 2023-24. A restoration of funding levels in 2025-26 may help reverse this trend in future, but budget allocation remains below 2022-23 in real terms.
Figure 5.1 Number of new affordable houses built in Scotland
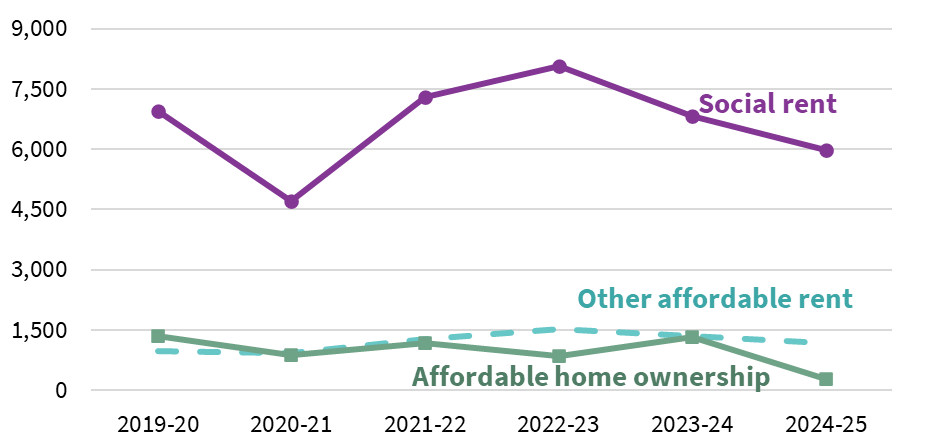
Source: Scottish Government (2025) (88)
The Affordable Housing Supply Programme is part of a suite of measures intended to help ease homelessness levels. As Figure 5.2 shows, homelessness levels have risen in recent years, with a small decrease in application numbers in the most recent data. These figures only capture homelessness that is reported – a 2025 Scottish Government report examines the additional challenge of “hidden homelessness,” in which people do not declare themselves homeless but are living in unsuitable, temporary situations (such as sofa-surfing with friends or sleeping in their car) or in an abusive situation (89).
Figure 5.2 Number of homelessness applications and applications citing rough sleeping in the previous 3 months
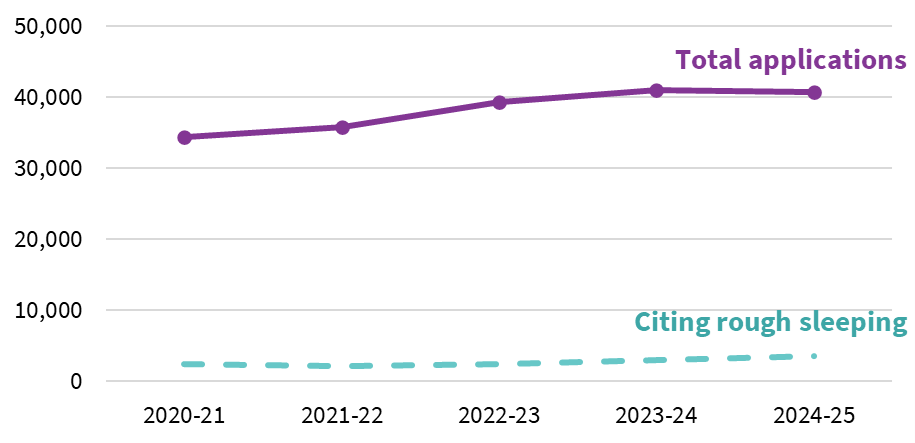
Source: Scottish Government (2025) (90)
Despite a slight decrease in homelessness applications in the most recent year, the overall rise in homelessness has led to an unprecedented number of families in Scotland living in temporary accommodation. A 2025 report by Shelter Scotland documents families’ experiences of temporary accommodation, highlighting multiple issues, including cramped conditions, broken (or absent) heating systems, limited facilities (for example, for laundry), infestations, and concerns about neighbourhood safety:
“It’s so small, the rooms are literally just like that basically. I can’t even put anything other than a bed.”
13-year-old participant (91)
“In the winter it is very, very cold, very cold. And always this [health] is affected, I take him into hospital. I tried to open, because all the heaters don’t work, I just have, like, a heater, I buy it from Home Bargains. […] This is very expensive and the house is very cold, in winter.”
Mother of children aged 13 and 17 (91)
“Nowhere to wash our clothes”
Mother of children aged 10 and 5 (91)
“Within the first three months, there was a moth infestation. The carpet had a hole in it had been eaten, but a cupboard had just been placed on top. And I had been like, what? Where are all these moths coming from? Till I moved everything. […] I had rats […] My son […] ended up back in hospital with an infection that comes from animals. And he had been in hospital for two weeks ill. It did hit his chest again, yeah, to get help, to get rid of the rats, was almost near impossible.”
Mother of 4-year-old child (91)
“I had thumping music on at all hours, and to go to school after that, it’s just like so annoying. And also, you don’t really feel safe because you can’t exactly go and ask him to turn the music down or something, because he’s got lots of mental issues. And also the person next us in the flat, I don’t know, just doesn’t feel very safe. We were on the outskirts of the town we were in, but it wasn’t a safe town.”
15-year-old participant (91)
The consequences of this, as described by participants, include direct mental and physical health problems, social isolation (caused by regular moves and having accommodation that is too small to invite people into), and difficulties with accessing key public services (such as GPs or schools).
Another study released in 2025 noted variations in council support, highlighting that the quality of supported accommodation between, and within, councils seemed variable (33). In the year 2023-24 there were 7,400 households placed in temporary accommodation which was deemed by law to be “unsuitable.” These breaches of this law, the Unsuitable Accommodation Order, has increased over time, rising from around 6% of all households in temporary accommodation in 2022 to 12% in 2024 (92).
Mental health continues to be the most common reason for failing to maintain accommodation prior to a homelessness application. There has also been a notable rise in people citing physical health conditions as a factor, which has overtaken those citing drug and alcohol dependency (Figure 5.3).
Figure 5.3 Number of homeless applications citing mental health, physical health, or a drug or alcohol dependency
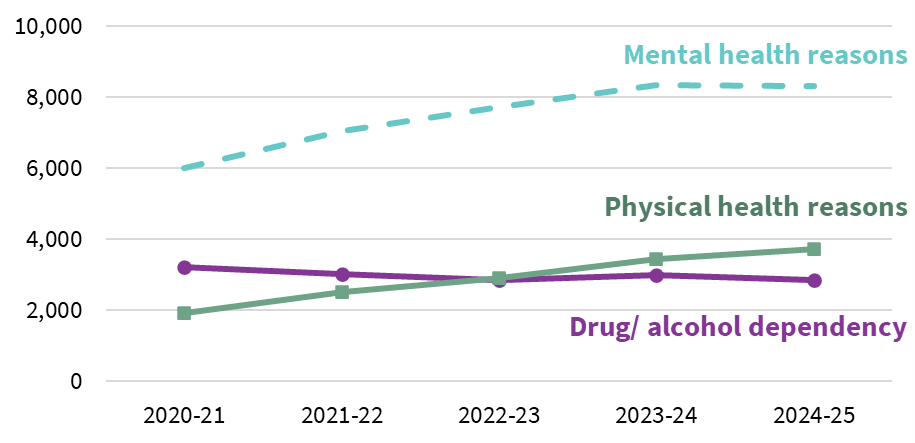
Source: Scottish Government (2025) (90)
A 2025 Scottish Government report exploring housing insecurity and hidden homelessness underlined the role that mental ill health can play in people’s pathways to becoming homeless:
“I was in a house with three kids with additional needs all in the one room. It was difficult. That wee boy was quite suicidal at the time as well, [he would] climb out windows and jump over bannisters and bring me knives [out the] drawers. It was difficult because he wasn’t getting his own space to regulate. So, we’re all very on top of one another and [it was] very frustrating.”
Participant (89)
On a more positive note, the number of estimated and identified deaths amongst people experiencing homelessness continued to reduce slightly in the latest data for 2023. These statistics include people experiencing rough sleeping as well as in temporary accommodation (Figure 5.4).
For people who are not homeless, the quality of homes that people on low incomes live in remains an issue of concern, with damp and mould in particular presenting health hazards. Data on housing quality was disrupted during the pandemic but, with two subsequent waves of data from the Scottish Housing Conditions Survey which are comparable to pre-pandemic data, we can once again monitor changes over time.
In the private and social rented sector, there has been deterioration in housing conditions, with an increase in reports of damp and condensation (Figure 5.5). The same survey reports an increase in mould within the private rented sector over the same time period.
Figure 5.4 Number of estimated and identified deaths among people experiencing homelessness
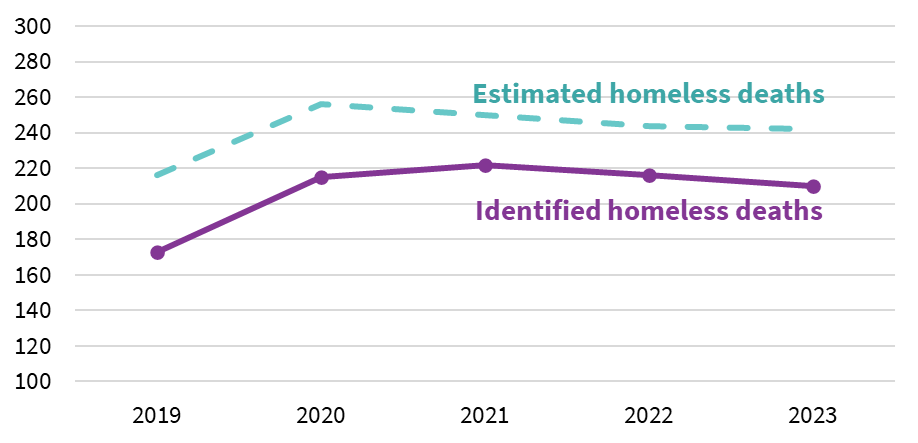
Source: National Records of Scotland (2024) (93)
Figure 5.5 Proportion of housing stock with damp or condensation by tenure
Source: Scottish Government (2025) (94)
Note: Data from the years 2020 and 2021 are not available due to the COVID-19 pandemic.
As well as directly impacting people’s health, qualitative reports highlight how stressful living with damp and mould can be and note the material consequences of having to replace items that become mouldy:
“I moved from a flat to a house and the standard of living just went up extremely because, in the flat there was mould and damp on the walls. It was terrible living conditions. Anything you bought, like materials, after a while the damp would just sit into it and you’d have to get rid of it, because it was unbearable.”
Participant, age 17(33)
Being able to heat a home sufficiently is a further safeguard against poor quality homes. Rates of fuel poverty (based on the proportion of a person’s income required to heat a home and the residual income after fuel costs are deducted) continued to rise in the latest data, at 34% in 2023 compared to 25% in 2019.
An update on the impact of the rent cap
The Scottish Parliament is progressing a Housing Bill that includes Awaab’s Law, named after Awaab Ishak, who died in 2020 in England from mould exposure. The measure would set time limits for social landlords to investigate disrepair and start repairs. Similar duties are not currently planned for the private rented sector, even though these problems are often more prevalent there.
The Bill also proposes rent controls, allowing the Scottish Government to designate rent control areas based on evidence from local authorities. In our September 2024 Inequality Landscape report, we considered whether the rent cap, in place from October 2022 to end March 2024, might be driving relatively lower housing costs in Scotland. Preliminary data at that time (up to the end of 2023) showed private sector rents declining in Scotland, whilst remaining fairly flat in the rest of the UK.
Now we have data up till the end of 2024, and we do not see a continuation in the divergence between Scotland and the rest of the UK, which we may expect if the rent cap was having a significant impact on rents in Scotland. This suggest that the rent cap, which continued through to the end of 2024, may not have been the main driver of the previous reduction. As we noted in our 2024 Inequality Landscape Report, Scotland does not have good enough data on rents to analyse the impact of the rent cap more rigorously.
Figure 5.6 Weekly housing costs in the private rented sector
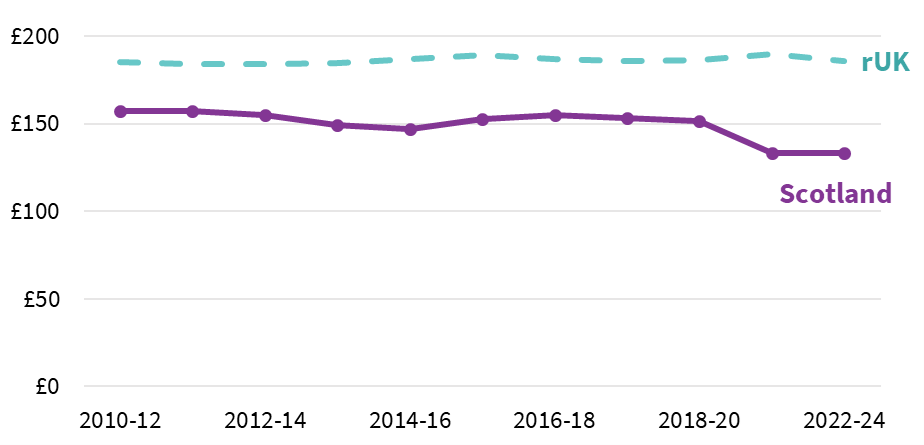
Source: SHERU analysis of DWP (2025) Households Below Average Income (HBAI) (95)
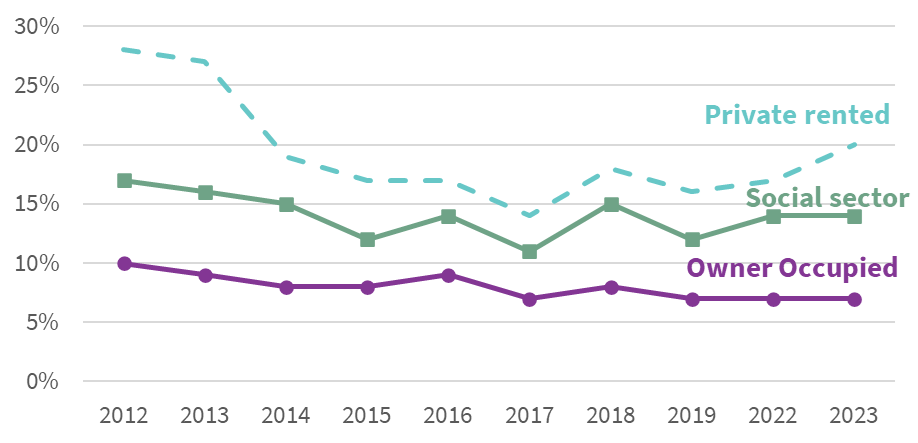
The main inequalities in terms of housing in Scotland remain between different tenures; those who rent tend to be poorer and, as seen above, are more likely to be living in poorer quality homes. Poverty rates within the social rented and private rented sectors are trending downwards but remain much higher than for owner occupiers (Figure 5.7).
Rates of food insecurity for people in the private rented sector have come down from their peak last year, while in the social rented sector they remain at about the same rate as last year. Levels of food insecurity among owner occupiers are much lower than in the two rental sectors (Figure 5.8).
Figure 5.7 Proportion of population in relative poverty by tenure
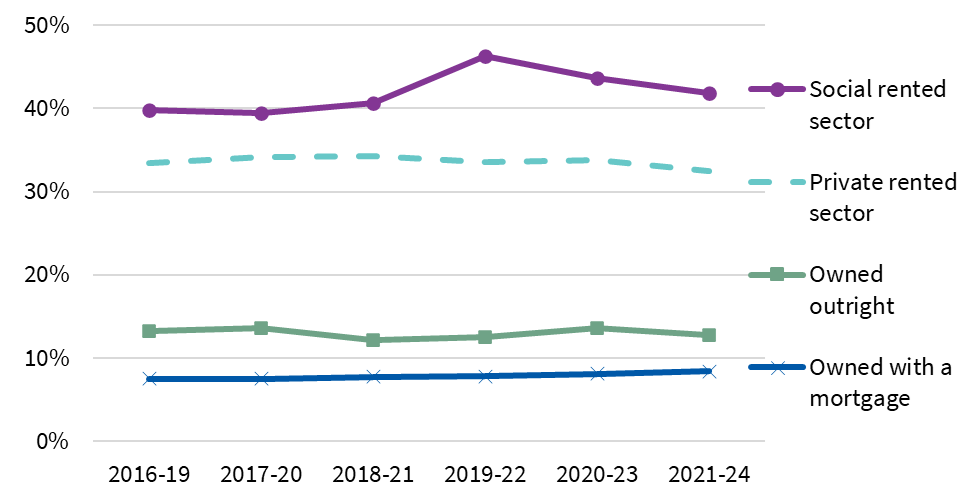
Source: Scottish Government (2025) (32)
Figure 5.8 Proportion of people that are food insecure by tenure
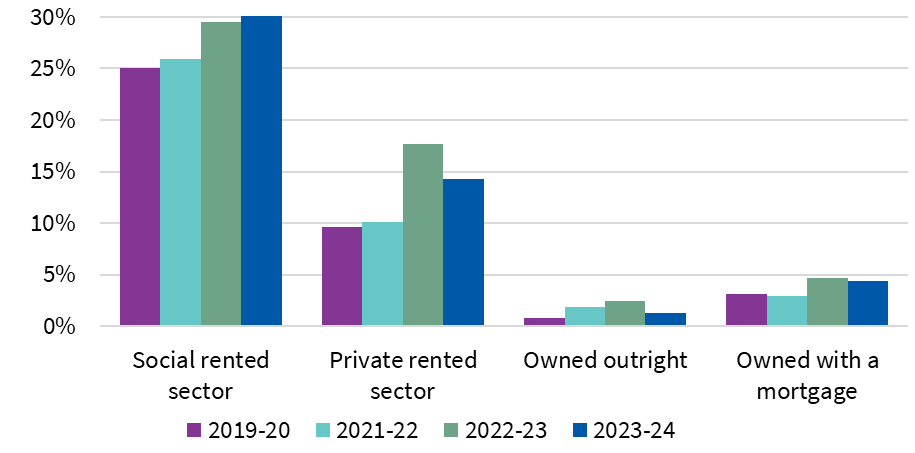
Source: SHERU analysis of DWP (2025) Households Below Average Income (HBAI) (95)
The Scottish Government’s ambitious Housing to 2040 strategy sets out a long-term vision for ensuring that everyone in Scotland has access to a safe, good-quality, affordable home that meets their needs and supports wellbeing. There are multiple references to addressing inequalities and disadvantage within Housing to 2040 and this strategy has the potential to help reduce health inequalities. Key actions include preventing homelessness, improving housing standards and retrofitting homes for energy efficiency. Some of these commitments are incorporated into a new Housing Bill, which is currently progressing through the Scottish Parliament.
Yet, while the ambitions in Housing to 2040 and the linked Housing Bill are commendable, major questions are being raised about its potential to realise the strategy’s vision, as we discuss in more detail in Raising the roof: Can Scotland’s Housing to the 2040 Strategy help as an approach to reduce health inequalities? (96). Since June 2023, 13 of Scotland’s 32 Local Authorities have declared a housing emergency. In May 2024, the Scottish Parliament recognised that Scotland was facing a national housing emergency. Calls for clearer implementation plans for achieving the key commitments have been growing. For the moment, the political commitment to ensuring people have access to “affordable housing” is being questioned in light of limited resources. Assessing the implementation of Housing to 2040 will continue to be a core focus for SHERU in the coming year.
Part 2: Reducing preventable deaths from drugs, alcohol and suicide – the role of socio-economic determinants
People in Scotland are more likely to die from drugs (6), alcohol (7), or suicide (8) than any other country in the United Kingdom. Even worse, Scotland has the highest drug-related mortality rate in Western Europe, and among the highest mortality rates from alcohol and suicide (97,98).
The issue is most acute for men in Scotland. In 2023, 70% of the people who died from drugs, alcohol, and suicide were male[1]. Since 2001, the cumulative effect of these three outcomes has grown over time, driven largely by dramatic increases in drug-related deaths. And, while deaths from alcohol and suicide are lower than they were nearly 25 years ago, neither has seen much change in the last decade.
Figure 6.1 Age standardised mortality rates for men from alcohol, drugs and suicide (per 100,000 population)
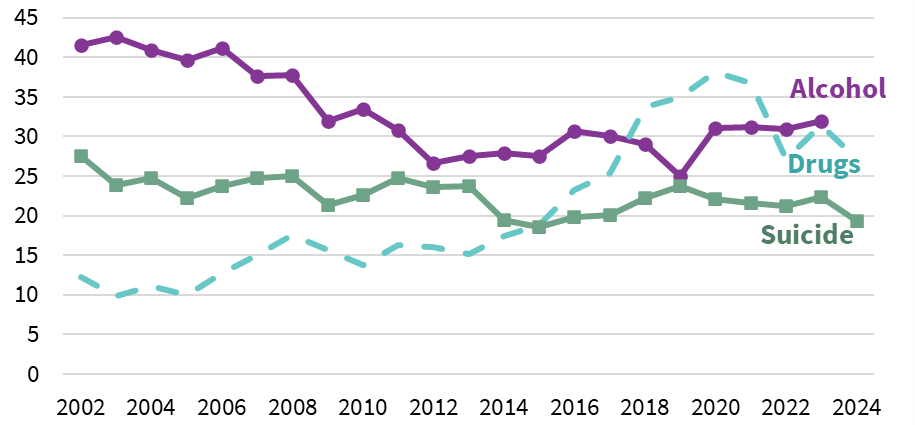
Source: SHERU analysis of National Records of Scotland (2024) Drug-related Deaths, Probable Suicides, and Alcohol-specific deaths (6,29,99)
Suicide, especially among younger populations, has been described as “[…] the ultimate expression of disaffection and alienation” and a “measure of our collective mental and social wellbeing” (100). Similarly, harmful consumption of alcohol and drugs have long been shown to be associated with a sense of powerlessness and social alienation (101,102). In short, where deaths from suicide, drugs and alcohol are high and rising, it suggests something is going deeply and acutely wrong for that population. For this reason, these three causes of death are sometimes collectively referred to as “deaths of despair” (103). This term highlights the fact that deaths from suicide, drugs and alcohol are often shaped by social and economic conditions that accumulate in ways that cause people to experience a strong sense of despair.
Factors associated with preventable deaths from drugs, alcohol and suicide include trauma (including in childhood), poverty, poor educational experiences, unemployment, the breakdown of interpersonal relationships and homelessness (87,104–106). People who are have prior interactions with the criminal justice system are also disproportionately represented in the statistics on deaths from drugs, alcohol and suicide in Scotland, with men in prison being a much higher risk of death from suicide and drug use compared to men in the wider community (107,108), suggesting that it is important to consider the role of the Scottish justice system in perpetuating harm.
Scotland is an extreme example of the socio-economic inequalities associated with deaths from drugs, alcohol and suicide: people living in the most deprived 20% of the country accounted for nearly 40% of all deaths from drugs, alcohol or suicide in 2023. Nearly a quarter of all people dying from alcohol and suicide[2] in 2023 were men living in the most deprived Scottish neighbourhoods[3] – a group which only makes up about one-tenth of the total Scottish population. (6,29,99)
There is also a regional element to this picture. Mortality rates from suicide are highest for men living in remote small towns, followed by urban areas, and are low among rural communities. Alcohol mortality is highest in urban areas but is closely followed by remote small towns. Data for drug mortality based on urban/rural classification is not available. Regional differences are further reflected in local authority data (Map 1).
Table 1 Age- and sex-standardised mortality rates (per 100,000 population) among men for alcohol and suicide, 2021-2023 average
Source: NRS (29,99)
Map 1 Alcohol, drug, and suicide mortality rates (age-sex standardised rates per 100,000 population) by local authority, 2019-2023
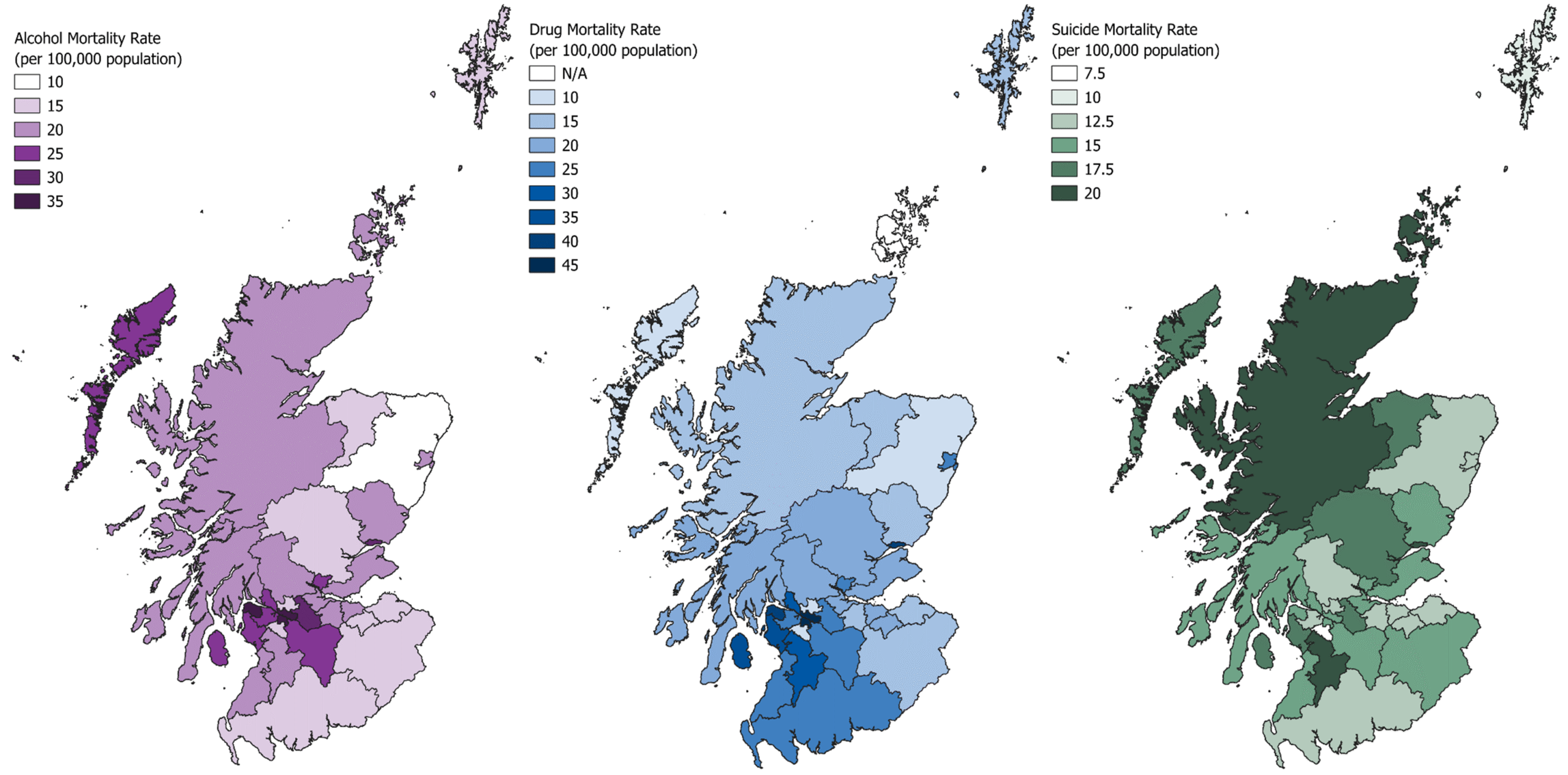
Source: NRS (6,29,99)
In general, there is not consistent overlap between the three maps. Drug and alcohol mortality tend to affect urban local authorities more: Glasgow and Inverclyde have the highest rates of drug and alcohol mortality, although they fall out of the top third for suicide mortality rates. West Dunbartonshire and North Ayrshire also follow this pattern, with high drug and alcohol mortality rates and roughly average suicide rates.
Suicide affects rural local authorities more. On average across 2019-2023 (our last period with comparable data), Highland, Orkney, and Moray all had high suicide mortality rates and relatively low drug and alcohol mortality rates, whilst East Ayrshire had a high drug and suicide rate, and Na h-Eileanan Siar had high alcohol and suicide mortality rates.
Dundee city is the one region that falls into the top across each measure. Dundee had the highest suicide rate in Scotland, at 21 deaths per 100,000 population. Dundee also had the second-highest drug mortality rate and the fourth-highest alcohol mortality rate.
All of this contributes to the fact that men in Scotland have the shortest life expectancy in Western Europe, with substantial inequalities in life expectancy based on socio-economic conditions. Men in the most deprived[4] parts of Scotland live an estimated 13.2 years fewer than men in the least deprived regions (4). Deaths from alcohol, drugs and suicide play a substantial role in absolute inequalities in mortality in Scotland (109), in addition to the broader contribution that alcohol and drug use make to inequalities in avoidable, preventable deaths from other causes (Figure 6.2) (110).
Figure 6.2 Avoidable, preventable, and treatable deaths

Source: National Records of Scotland (2025) (110)
We know that, in Scotland, the group with the highest rates of substance related deaths and deaths from suicide are men in their 40s and 50s, although a considerable number of deaths happen before this point. We are interested in the socio-economic status of men in the years prior to these deaths occurring which we have broadly determined as men aged 18-44. The socio-economic circumstances of men at this stage of life appear to be an overlooked area in Scottish research and policy – a policy blind spot – as we explore further below.
Policy blind spots emerge from a complex interplay of factors, including political ideologies and priorities, regulatory and governance frameworks, data gaps, limited advocates or policy influencers prioritising the topic, and a lack of external (e.g. media) attention. Policy blind spots are also shaped by historical decisions, fiscal spending, and decision-making authority (in Scotland, for example, authority can sit at UK, devolved or local level and, for some issues – including alcohol and drugs – it is a complex mix). Recognising these factors is key to identifying where policy may be missing, poorly designed or not effectively delivered across different levels of government (111).
Our assessment is that policy currently places limited emphasis on improving men’s socio-economic circumstances earlier in life to prevent crises later on. After age 16, when young men start to leave full-time education and the family home or care setting, there are few safety nets designed specifically to support them when things go wrong.
There are touchpoints that could help identify and support younger adult men, such as employability services and the social security system. However, these services often prioritise groups that with only limited overlap with men aged 18- 44. For example, Scotland’s flagship approach to employability, No One Left Behind, prioritises parents returning to work, lone parents, and those at risk of child poverty (112), and the devolved social security system is heavily focused on family and child benefits, including the Scottish Child Payment. While many men – especially fathers – are covered, single adult men not living with children often fall between priority groups. Often, it isn’t until something goes badly wrong that services start engaging. For example, police call outs, homelessness applications, accident and emergency services and drug, alcohol or mental health services. This could not be further from the preventative approach that is supposed to be at the heart of Scottish policy making.
Of course, these issues do not just affect men. Women account for around a third of deaths from alcohol and drugs in Scotland and a quarter of deaths from suicide. Women are also more likely to attempt suicide, although data on suicide attempts is limited and not always reliable – it can be hard for professionals to distinguish a suicide attempt from others forms of self-harm and ongoing stigma means that people may not disclose suicide attempts in surveys. In 2021, the Scottish Health Survey reported that 7% of adult women said they had ever attempted suicide, compared to 6% of adult men (113). More recent data on attempts has not been published. Women also account for a third of the number of people seeking treatment for drug and alcohol use.
Moreover, while deaths from alcohol and suicide have been relatively stable in recent years, deaths from drugs among women have (as with men) increased dramatically in the past two decades. And, as with men, women from more deprived areas are disproportionately represented.
The over-representation of people from more deprived areas in deaths from alcohol, drugs and suicide mean that the ripple effects (e.g. bereavements from these deaths among parents, siblings and friends) are also concentrated more among people living in deprived areas in Scotland. The children of those who die from drugs, alcohol and suicide will carry this trauma across generations.
Whilst acknowledging that it is not only men who are impacted by deaths from drugs, alcohol and suicide, we do concentrate the rest of our analysis on the socio-economic circumstances of men given their overrepresentation in the statistics on deaths from drugs, alcohol and suicide.
Pinpointing who is at greatest risk from substance related and suicide deaths in ways that enable targeted preventative action is challenging. When we look at data on living standards, things often look better for men than for women. This is not necessarily surprising: these are prime working years, and men between these ages have higher rates of employment and higher incomes – on average – compared to other groups. And yet, men are the most likely to die prematurely, the most likely to be homeless, and the most likely to be in prison. For deaths by suicide, there is also an association with rurality, with remote small towns having had the highest suicide rates, and large urban areas the lowest suicide rates, for most of the last decade (114).
The result is that, when data are averaged, men in Scotland often appear to be faring relatively well, and we fail to focus on the lives of men who are not doing well. This group is hard to capture in current data sources, and particularly hard to trace over time. This means it can be challenging to build a cohesive and comprehensive picture of the men who are dying early – their education levels, their relationship with the labour market, their income, or their family and social dynamics.
Focusing on men at risk of substance related and suicide deaths can unintentionally risk appearing to downplay the structural inequalities, discrimination and violence that far too many women in Scotland face. Yet, we see some evidence that the lack of attention paid to the welfare of young adult men in Scottish research and policy is beginning to be problematised by some such men:
“I think we’re the most criticised group of folk, but we get the least amount of credit out of any sort of…demographic type, you know what I mean?”
James (115)
There are a small number of qualitative sources that focus on men facing particular forms of disadvantage in Scotland but each of these only provides insights into very specific groups and socio-economic factors. In this report, we synthesise some of this evidence to explore how socio-economic factors coalesce across the lifecycle to increase the risk of death from suicide, drugs and alcohol by piecing together cross-sectional data.
We focus particularly on men’s experiences once they leave formal education and are outwith Scotland’s system of child services. This is not to downplay what happens within childhood or during youth transitions to adulthood. As we acknowledge below, experiences in early life have direct health impacts and are often critical in shaping people’s experiences throughout adulthood. For example, the following extract illustrates the crucial role that traumatic childhood experiences can play in substance use:
“… there’s a lot of stuff going on in my house that I see as a young kid and it makes me scared, makes me feel of fear, and I can’t be, trust the people that are meant to love me. I don’t feel safe.”… “And this fear gets worse and worse throughout my lifetime”… “Never knowing what’s going to happen and when I find that first substance, just takes all that stuff away. Makes it easier. The best way I could describe it.”
Jack, 49 (116)
The above extract reflects the way in which children’s experiences and social outcomes (including their living standards) can be directly shaped by the situation of, and their relationships with, their parents. Around 90% of non-resident parents in Scotland are men; on average between 2021-2024, 64,000 men did not live with their child(ren). A 2017 study found that around 16% of children responding to a survey in Scotland had a poor relationship with their father, compared to 8% of respondents reporting a poor relationship with their mother (117). We also know that spending time in the Scottish care system – much more likely for children in deprived areas (118) – increases people’s likelihood of experiencing homelessness (119), unemployment (120), and poor health outcomes in adulthood (121).
It is important to acknowledge this ongoing interaction across generations. If Scotland achieves its stated ambitions of eradicating child poverty (for instance, via the Child Poverty Act) and ensuring that every child and young person who is care‑experienced grows up “loved, safe and respected” (as The Promise Scotland (58) declares), younger generations should fare much better as adults. Indeed, this would be an excellent example of preventative action.
However, in contrast to the strong policy focus on improving childhood and supporting young people, particularly those who are care-experienced, the welfare of young adult men currently seems to be something of a policy blind spot. This is important because we currently have a generation of young adult men with relatively high experiences of childhood poverty. What happens in adulthood may either ameliorate or worsen the impact of childhood experiences. If Scotland is serious about reducing deaths from drugs, alcohol and suicide, we need to better understand this population group and ensure that those at risk receive the necessary support earlier.
In focusing on men in early adulthood (18-44), we look at three areas (Figure 6.3). First, indicators and policy related to living standards, primarily those that contribute to income but also broader factors that relate to societal wellbeing. The types of policies that can improve these factors sit in the “primary prevention” space, supporting people before poor (health) outcomes have occurred.
Figure 6.3 Situating the factors analysed in our report
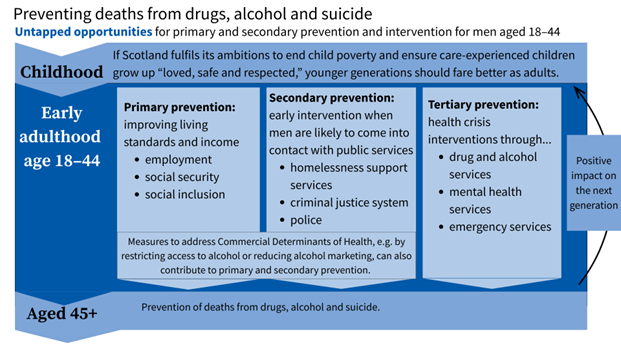
Second, we examine some of the adverse outcomes that occur for this population: homelessness and interactions with the criminal justice system. At this point, for many people, addiction and mental health issues are already prevalent. We present these as opportunities for early intervention because they are points at which men are likely to come into contact with public services. This provides a chance to offer support to prevent further escalation of harm.
We frame crisis interventions related to drug and alcohol services, mental health services and emergency services, as tertiary forms of prevention – these services commonly play a role in trying to prevent deaths from alcohol, drugs and suicide when people are already experiencing an acute crisis. These are less the focus of our analysis since this is the most “downstream,” responsive form of prevention. However, we know that most people engaging with drug and alcohol treatment services are men. In 2023-24, around 11,000 men sought treatment for drugs, alcohol, or both (122).
Other types of policy that are also outwith our analysis, include behavioural interventions, which are embedded within existing strategies[5] and policies that aim to address the commercial determinants of health (e.g., to restrict the availability or marketing of alcohol, which we briefly summarise in Box 2). Our focus is on the socio-economic conditions that shape the high and unequal patterns of early deaths across harmful substance use and suicide in Scotland, where our sense is that evidence, advocacy and policy action remain both more limited and more fragmented.
In the final part of this deep dive into the socio-economic drivers of deaths attributable to harmful substance use and suicide we look at some international evidence to showcase three examples in which other countries have successfully implemented joined-up approaches to preventing the type of poor health outcomes that are so prevalent for men in Scotland.
Preventative action via commercial determinants of health in Scotland
In Part 2 of this report, our approach has been to consider socio-economic factors that contribute to deaths from alcohol, drugs and suicide. It is important to acknowledge that there are other policy actions, related to commercial determinants of health, that try to reduce the harms caused by alcohol in Scotland by restricting the accessibility of cheap alcohol. These build on earlier tobacco control efforts – most notably, Scotland’s pioneering ban on smoking in public places, which gained Scotland a reputation as a public health leader (123).
Alcohol availability and marketing have been addressed through: (1) a requirement for alcohol licensing decisions to consider public health objectives, with the potential for local licensing boards to reject applications for new alcohol premises on the basis of overprovision; (2) the Alcohol etc. (Scotland) Act 2010, which restricts some alcohol promotions and bans off-trade multi-buy deals on alcohol; and (3) Minimum Unit Pricing (MUP), which was legislated in 2012 and implemented at 50p per unit in May 2018, uprated to 65p on 30 September 2024.
Together, these measures form a distinctive package designed to curb very cheap alcohol, limit promotion-driven marketing and reduce inequalities in local availability. Independent evaluations suggest that MUP and the multi-buy ban have reduced alcohol sales and contributed to declines in alcohol-related deaths and hospital admissions (124,125). It is therefore reasonable to conclude that mortality would have been higher without these policies. By contrast, the requirement for Licensing Boards to consider public health has, to date, had a more limited and uneven impact on availability (126). The availability of alcohol in Scotland remains, like tobacco, unequally distributed, with more deprived (especially urban) communities facing higher exposure (127). To be tackled effectively, alcohol harms and deaths will require actions that reduce the exposure and availability of alcohol, alongside measures to address the socio-economic disadvantages set out in this report.
[1] In 2023, 3,239 people died from alcohol-specific causes, probable suicides, or drug use. 2,255 of these deaths were men (6,29,99)
[2] Drug-related mortality rates are not published by gender and SIMD quintile, although 69% of drug related deaths were male, and 48% were from people of both genders living in the most deprived 20% of Scotland.
[3] Defined as the 20% most deprived areas according to the SIMD.
[4] Here meaning the most deprived 10% of neighbourhoods in Scotland compared to the least deprived 10%
[5] For example, see Public Health Scotland’s Alcohol Brief Interventions: A review of strategy and recommendations for policy
Understanding socio-economic determinants of health in early adulthood
The fact that men aged 18-44 do well, on average, masks issues facing a subset of men who face socio-economic exclusion
When analysing men aged 18-44, it’s crucial to consider the variance in outcomes. Men in this age group have on average higher rates of employment than any other age and gender group in Scotland. However, some men struggle to secure decent employment and we do not currently have sufficient insights to understand which policies and interventions might make the biggest difference. We do not, for example, have data that links education with mortality in Scotland, so we do not know how concentrated deaths from drugs, alcohol and suicide are among men based on their education levels, though we do know that in the UK, on average, adults with lower levels of qualifications tend to have lower income as young adults (128,129).
As we discussed in Part 1, recent labour market data which explores the reasons for why men are in and out of work is not robust enough to analyse at the moment. However, looking at regional data can be a useful way of getting underneath the “average” to see where there are variations between areas. For this analysis, we have used the 2022 Census. It is important to note that this data is not directly comparable to the questions asked about inactivity and unemployment in the Labour Force Survey, but it does provide us with a detailed regional analysis of areas where issues related to employment for men are concentrated.
Areas in the central belt and southwest have notably lower levels of employment among working-aged men who are not in education or retired (Map 2). On average, according to the 2022 census, remote small towns had the lowest rates of employment among men[1], followed by urban areas, whilst rural communities have the highest. Long-term illness or disability was the most common reason why men were not in employment, with around 8% of men in remote areas out-of-work for this reason (130).
This issue mirrors the mortality rates discussed in Table 1: remote small towns have the lowest employment levels for men, the highest suicide rates, and alcohol death rates that are much closer to urban levels than to other small towns or rural communities.
Map 2 Proportions of adult men that are either unemployed or economically inactive (excluding inactivity due to education or retirement) by ward, 2022, with areas with more than 25% of men out-of-work highlighted
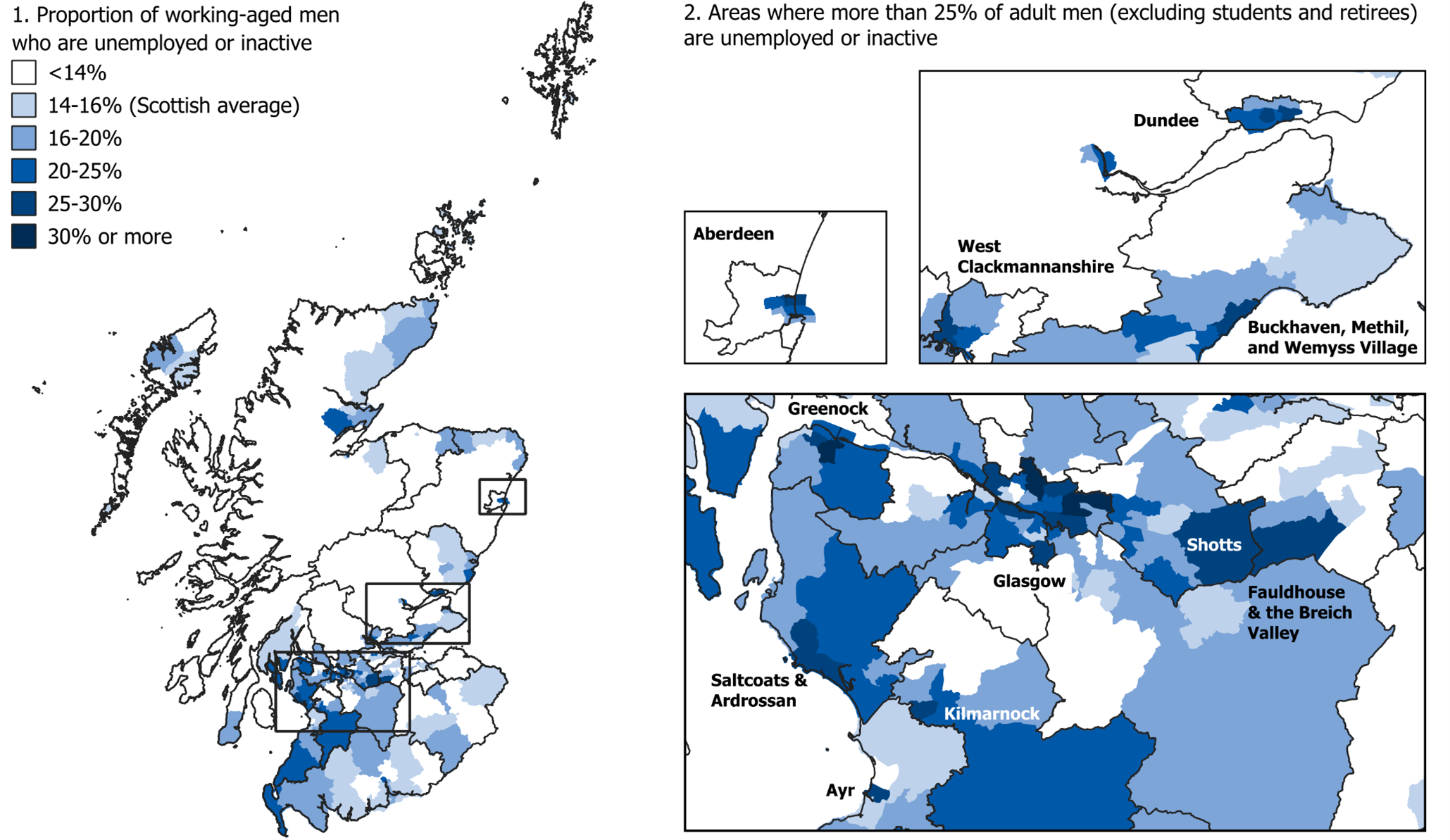
Source: 2022 Census (130)
Transitions from education into employment can be a particularly difficult time for some young men
There are glimpses in the data of issues adversely affecting some men. For example, around 5% of male students leave school without a positive destination, such as employment or higher education. There has been a significant reduction in those numbers over time, but things have plateaued in recent years (along with a significant Covid bump) (Figure 6.4).
Figure 6.4 Proportion of school leavers without a positive destination
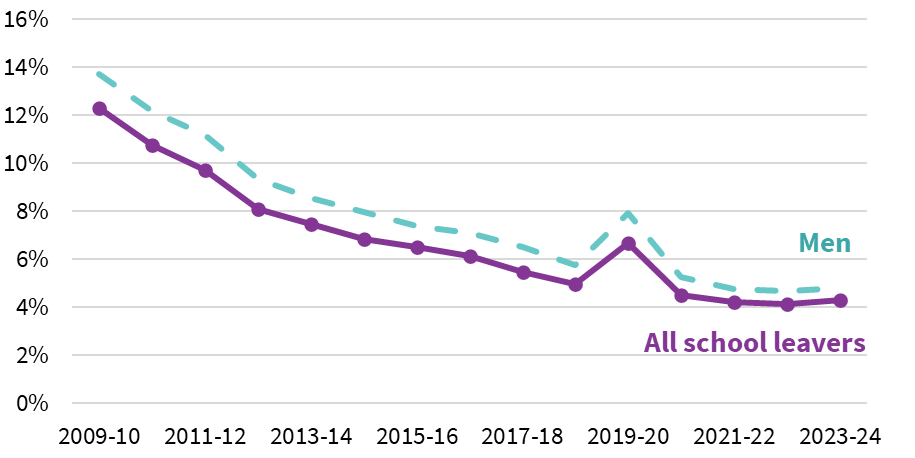
Source: Scottish Government (2025) (131)
A recent mixed methods study of young men’s education to work transitions in Glasgow and Liverpool includes multiple accounts of issues with finding work, with participants describing the negative impact on their mental health of experiencing repeated rejections. For example:
“And it’s not even that I’d get replies back, it’s just I wouldn’t even hear back off jobs I was applying for, that was just, made me not want to do it and I ended up sinking into a really deep depression during that time just because nothing seemed to be working out”
Ian, Glasgow (132)
Lack of financial security from work is a growing issue for younger adult men
Men between 16 and 19 are more likely than women to not be participating in education, employment or training (Figure 6.5).
Securing employment also does not necessarily mean financial security. Men are increasingly likely to experience insecure work. Since the late 2000s, men aged 18-24 have faced an unprecedented increase in non-permanent jobs (Figure 6.6).
The proportion of men working part-time has also increased over time, particularly for 18–24-year-olds. Different factors may be driving this change, some of which could be a deliberate trade-off to improve work life balance or to take on unpaid work such as childcare (Figure 6.7).
Qualitative insights suggest that these changes in employment are likely to be at least partially driven by available work. For example:
“it’s like you know, zero-hour contracts, minimum wage everywhere, and hardly anyone pays the living wage even, and I don’t see how they can validate that because there’s been no wage increase due to inflation like for ages”
Stevie, Glasgow (132)
“Everything’s temporary, like fixed term employment, or even if you’re not supposed to be fired, people just get fired for dumb reasons all the time”
Anthony, Glasgow (132)
Regardless of the reason, inequality in male earnings has increased in the last few decades (133).
Figure 6.5 Proportion of those aged between 16 and 19 who are not participating in education, employment, or training
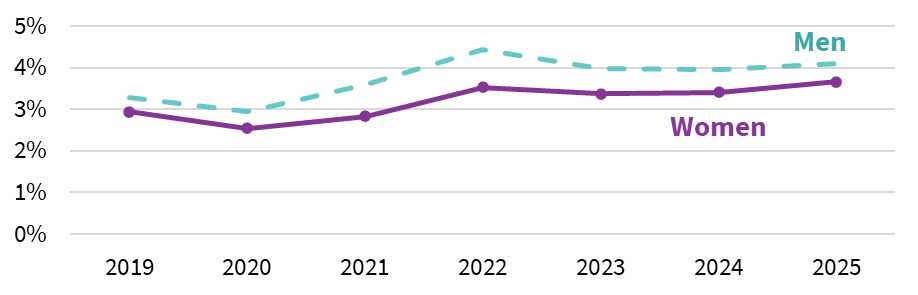
Source: Skills Development Scotland (2025) (73)
Figure 6.6 Proportion of adults who are not in education, working in jobs that are not permanent in some way, 3-year rolling average
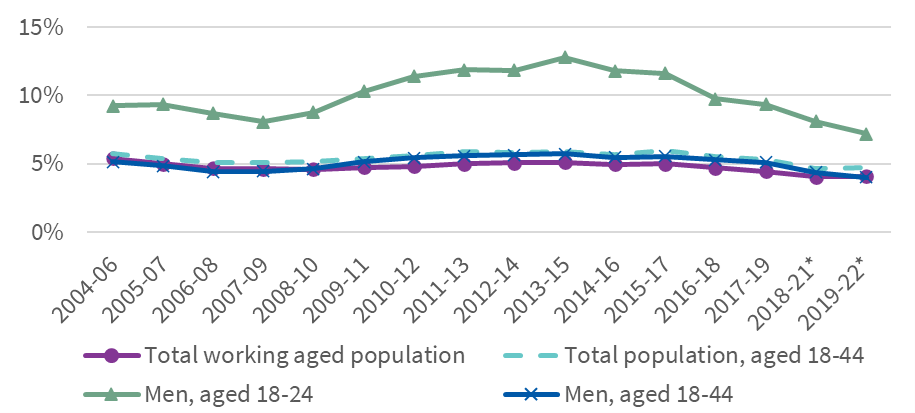
Figure 6.7 Proportion of adults who are in part-time work and not in education, 3-year rolling average
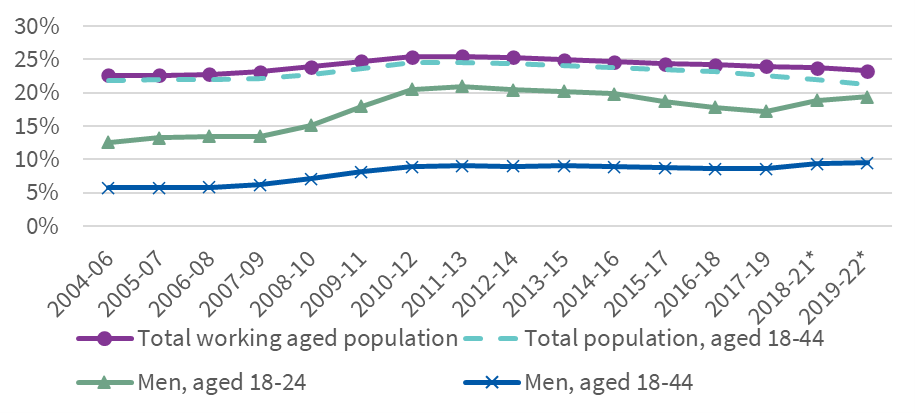
Source for Figure 6.6 and 6.7: SHERU analysis of the ONS (2004-2022) Annual Population Survey, January – December (134)
Note: 2020 is omitted due to data quality issues
The type of work is an important factor, and the ongoing legacy of deindustrialisation still affects younger adult men today
The type of work that adults undertake is also a predictor of health outcomes and of potentially unstable employment. The long-term impact of the reduction in jobs associated with heavy industry in Scotland has been well documented. Quantitative analysis of drug-related deaths in Scotland has found higher death rates in the 1990s among men aged 18-45, concentrated especially among those from the most deprived areas. The authors argue that this “[…] cohort effect is consistent with the hypothesis that exposure to the changing social, economic and political contexts of the 1980s created a delayed negative health impact” (135).
Qualitative research adds weight to this hypothesis, demonstrating that men’s experiences of deindustrialisation in Scotland has varied across generations, with implications for both employment and health outcomes. For older cohorts of men, loss of work in the context of the closure of large, industrial employers has often been identified as responsible for low self-esteem, shame, embarrassment and stigmatisation (136–139). With employment often being considered a core part of masculine identity, not having a job was experienced by some men as having “their life taken away from them” (138). For more recent generations of men, growing up in areas affected by large-scale deindustrialisation has often resulted in longer-term employment, a lack of sense of hope that a suitable job will ever materialise, and ongoing engagement with employment support services:
“The Job Centre, that turns my stomach. I gotta go there every fortnight, it’s only every fortnight, but still, leadin’up to that I can feel it in my stomach and my stomach turns and, y’know, it’s just not a pleasant experience for me … Well it’s called the job centre but I don’t think it actually tries to really get you a job. You go in there and they’ve got procedures and you’ve got to do what they want because they’ve got bosses on top of them and if they’re not seen to be doin’what you’re supposed to be doin’then they get intae trouble. I’ve got tae apply taea job every week, but if I can’t find a job I’m told I’ve tae send a CV tae any company, which I do to keep them right. If I don’t do that then they get intae trouble … So that just physically upsets me, and mentally.”
Owen, photovoice participant (136)
Men aged 18-44 are overrepresented in elementary occupations; associate professional occupations; process, plant, and machine operations; and skilled trades. Elementary occupations involve simple and routine tasks that typically require no formal qualifications or only basic training. These roles usually rely on physical effort or basic manual skills rather than technical expertise. They are often associated with a higher level of work-place injuries (138). Skilled trades occupations involve practical, manual, or technical skills, often acquired through apprenticeships, vocational training, or significant work experience. These roles require a higher degree of skill and autonomy than elementary occupations.
Figure 6.8 Proportion of people in each occupation group in their main job that are male and aged 18-44, 2018-2022 average
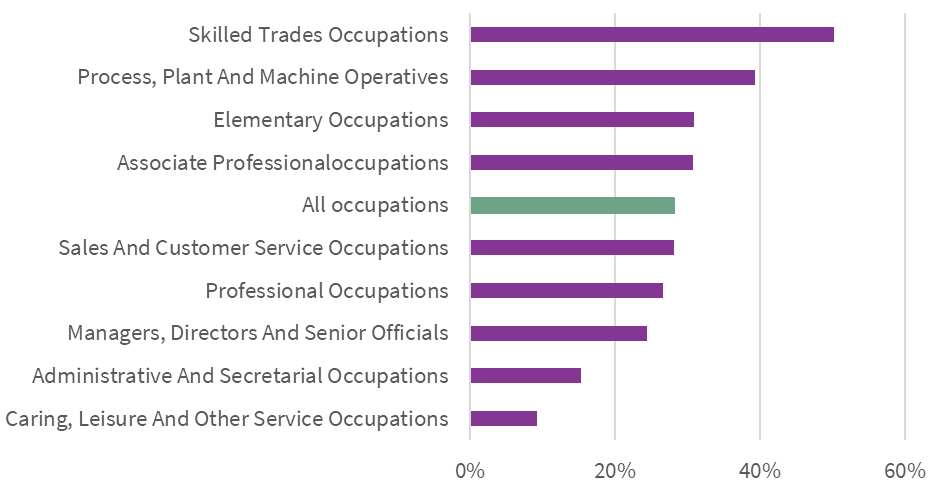
Source: SHERU analysis of the ONS (2018-19; 2021-22) Annual Population Survey, January – December (134)
Note: 2020 is excluded due to data quality issues
In some cases, younger employees might start off in less skilled roles and progress to more skilled roles, with more opportunities. However, a 2019 survey of people working in the Scottish construction industry found that around a third of respondents disagreed or strongly disagreed that they had opportunities for progression (140). More up-to-date research is needed to better understand options for career progression within key sectors, as well as to understand the threats posed by automation and AI technologies.
Process, plant, and machine operations; elementary occupations; and skilled trades faced relatively large drops in employment rates between 2008 and 2013, whilst other industries remained stable. Men working in elementary occupations also saw a dramatic decline in employment in the late 2000s and early 2010s, although with some recovery since. However, there are significantly fewer men in these age groups working in these jobs than there were in 2004-2006 and, whilst men in this age group have moved out of these industries more quickly than the population average, they have not moved into associate professional or other occupations more quickly either.
Figure 6.9 Proportion of adults currently or previously in selected occupations that are employed and not in education (3-year rolling average)
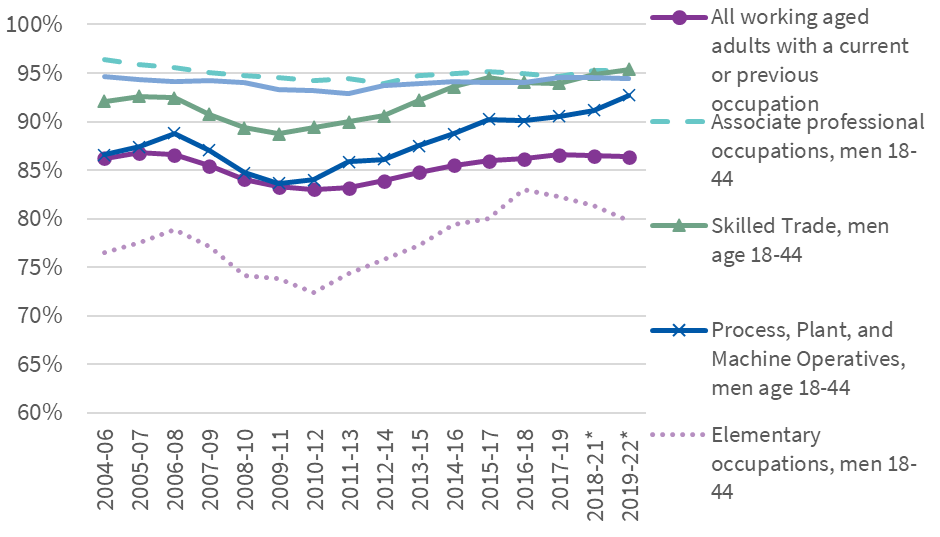
Source: SHERU analysis of the ONS (2004-2022) Annual Population Survey, January – December (134)
Note: 2020 is omitted due to data quality issues
Understanding the contemporary legacy of continuing deindustrialisation, particularly given that skilled trade and machine operations are at a high risk of automation, is an area that needs more research. Both qualitative and quantitative data that could help us understand the impacts on young adults in the past decade are limited. It is also unclear how employment patterns interact with other potential markers of socio-economic inequality, such as regional deprivation, immigrant status, and ethnicity, due to data quality issues.
We are unsure how well Scottish Government funded voluntary employment support is supporting younger adult men
In terms of Scottish Government policy intervention, it is difficult to see how this group are faring when they engage with Scottish Government funded voluntary employability services. Up to the age of 25 and after aged 50, more men than women are engaging with services, but for 25–49-year-olds, more women engage in services than men. This is at least partly due to the way that funding for No One Left Behind – the main employability funding pot in Scotland – is prioritised. As discussed earlier, services heavily prioritise parents who are out of work, which is more likely to be women between age 25 and 49. Statistics on progression into jobs isn’t disaggregated by age, but while men were more likely to enter employment overall (33% of male participants compared to 29% of female participants), the women that entered employment were slightly more successful at maintaining sustained employment than men (141).
SHERU is aiming to contribute to addressing some of the evidence gaps around employability over the coming year, as we examine the implementation of No One Left Behind and explore insights from peer-research and community accounts of efforts to secure paid work.
Health crises can also impact on employment
As people get older, the relationship between work insecurity, health and other social challenges can be bi-directional. For example, qualitative research exploring the life histories of older drug users in Scotland suggests that people who use drugs often become trapped in a cycle in which they struggle to secure (or maintain) employment and then engage in criminal activity to obtain the money required to buy drugs – a cycle which becomes hard to escape, especially where a criminal record ensues:
“I was a trainee engineer but through addiction and through the consequences of my action, I lost that job. Well, I couldn’t hold a job then and because I- I was so angry. I was against the authority. […] And then I’m not getting any qualifications. The only means I know making money is to doing wrong things and that selling drugs, committing crime, getting caught up in gang violence.”
Arthur, 47(116)
There are also growing concerns over economic activity linked to long term ill health and disability and a need to better understand the role of drug and alcohol use in this. Issues with data from the labour force survey (see Part 1) mean it is hard to draw any definitive conclusions about the most recent data. However, there has long been higher inactivity attributed to permanent ill health or disability for men aged 25-49 than is the case for older men, aged 50-64, or for women of any age (142).
Barriers to earnings from employment are closely linked to low income and poverty
Earnings are a key contributor to income and living standards and, given higher rates of employment on average, household incomes for men within this age group are notably higher than the Scottish average. However, we can trace some of the issues facing subsets of men in the labour market through to earnings for people in poverty. Over time, earnings as a share of income for men aged 18-44 (excluding students) has diverged from the population average, indicating that the earning potential for men aged 18-44 is being constrained.
Figure 6.10 Employment earnings as a share of income for people in poverty, indexed to 1994-96
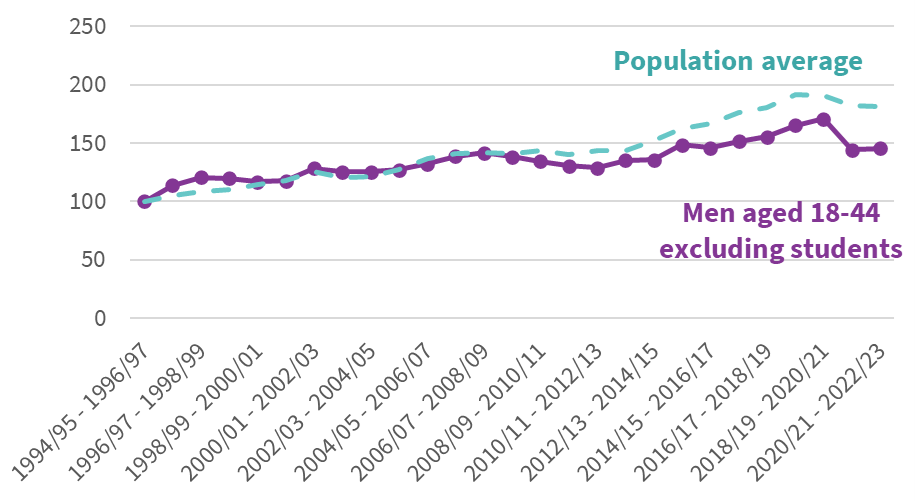
Source: SHERU analysis of DWP (2025) Households Below Average Income (HBAI) (95)
Social Security policy is not targeted at younger adult men
At the same time as seeing constraints on earnings, support from the social security system has not kept pace with the rest of the population.
Women are disproportionately represented in statistics on the social security system, both when considering working age out of work benefits (56% of caseload are women) and working age benefits available to those in and out of work (55% of caseload are women) (143). Women experience lower earnings on average and are more likely to live with a dependent child, leading to more women being eligible for support. However, for men who do rely on the social security system, we know that there has been little direct policy aimed at improving living standards for working aged men.
For the last few decades, there has been a significant level of policy focus across all levels of government on tackling child poverty and poverty among pensioners. This includes a recent Scottish Government policy focus on priority families[2] as well as the statutory child poverty targets (144). Focusing on these areas make sense, given the well-evidenced risks and harms that families face when experiencing poverty. However, this focus also means that men on low incomes who do not live in households with children are less likely to benefit from current policies to tackle poverty.
Post-2010 policy changes at UK Government level are also likely to have disproportionately negatively impacted on young adult men. One notable change was the removal of the automatic entitlement for people under the age of 35 to receive housing benefit or Universal Credit support for the cost of renting a self-contained one-bedroom flat. Instead, most single adults under-35 without dependants are now only eligible for support equivalent to the cost of a room in a shared house under the Local Housing Allowance (LHA) rules (145). Under 25s also have lower standard allowances in Universal Credit, continuing a pattern embedded in legacy benefits such as Jobseeker’s Allowance.
The Household Below Average Income dataset shows average benefit income for households including men aged 18-44 has fallen behind the population. In fact, mean income from benefits for men aged 18-44 is lower in real terms now than it was in the mid-1990s in contrast to the rest of the population where income from benefits has risen over the same time period (95).
Figure 6.11 Mean weekly income from benefits
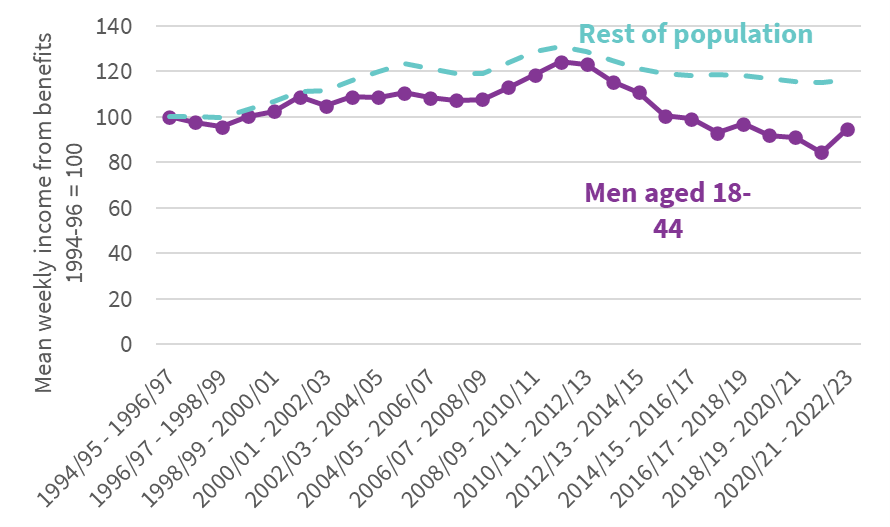
Source: SHERU analysis of DWP (2025) Households Below Average Income (HBAI)(95)
Growth in average income for younger adult men has struggled compared to the population average over the last two decades (if not before)
Taking earnings and social security together (along with income from other sources) poverty rates have risen for 18–44-year-olds over the last 40 years, a period during which they have fallen for the population as a whole. Since the mid-1990s, the poverty rate among men aged 18-44 has risen from an average of 18% between 1994 and 2000 to 20% between 2019 and 2024. Across those same time periods, the overall poverty rate among the Scottish population dropped from 23% to 20%.
Pre-1994, we can’t separate men and women in income data, but if we look at single adult households, sustained deterioration in income relative to the rest of the population starts in the mid-1980s and, by the early 1990s, average income for people entering young adulthood had dropped significantly compared to the generation born 5 or 10 years earlier (146).
Data limitations are an issue for analysing men from ethnic minority backgrounds, but there are reasons to be concerned
Men from ethnic minority backgrounds are a particular concern when it comes to poverty. Excluding men in full-time education, between 2021 and 2024, 45% of men aged 18-44 from ethnic minority backgrounds[3] were in poverty, compared to 17% of white men. The poverty rates for men from ethnic minority backgrounds fell significantly in the 1990s and early 2000s, but these men are still overrepresented in poverty data. Again, excluding men in education, 25% of all men aged 18-44 in relative poverty were from ethnic minority backgrounds in 2021-24. By comparison, only 12% of all men aged 18-44 were from minority ethnic backgrounds over that same period (95).
Scotland does not publish data on deaths from drugs, alcohol, or suicide by ethnicity, nor does it hold good data on health outcomes by ethnicity in general, meaning that we do not have a good sense of how poverty affects health outcomes for this group. Often, deaths related particularly to substance use are thought to be a problem concentrated among white men who have experienced socio-economic deprivation but, as Scotland becomes increasingly diverse, this may not remain the case.
Men aged 18-44 in poverty are more likely to face social exclusion
Social and familial dynamics throughout individuals’ lives are key predictors of long-term health outcomes. A study in Canada, for instance, found that there was a consistent relationship between social fragmentation, wherein people have low levels of community integration, and deaths due to alcohol, drugs, and suicide (147). More generally, social isolation and loneliness are correlated with early mortality (148).
There is also a strong intersection between mental ill health, trauma, and addiction in Scotland, with many people who use drugs over long periods attributing this at least partially to an effort to cope with traumatic experiences (116).
Quantifying integration into a community is difficult but there are notable differences between adults in poverty and those not in poverty. As shown in Figure 6.12, men aged 18-44 generally saw friends or family, or went out socially, slightly more than the average for working aged adults in 2023, and men in lone adult households went out socially more than the working aged average. Comparing adults in poverty, however, men in lone adult households fare notably worse than average. In 2023, only 55% of men aged 18-44 in lone adult households that are in poverty said that they go out socially monthly, and 77% say that they see friends or family monthly, far lower than the 95% reported for the same age group of men who are not in poverty, and also lower than the average for all working aged adults in poverty (85%).
Figure 6.12 Inequalities in the proportion of adults going out socially or seeing friends/family monthly, 2023-24
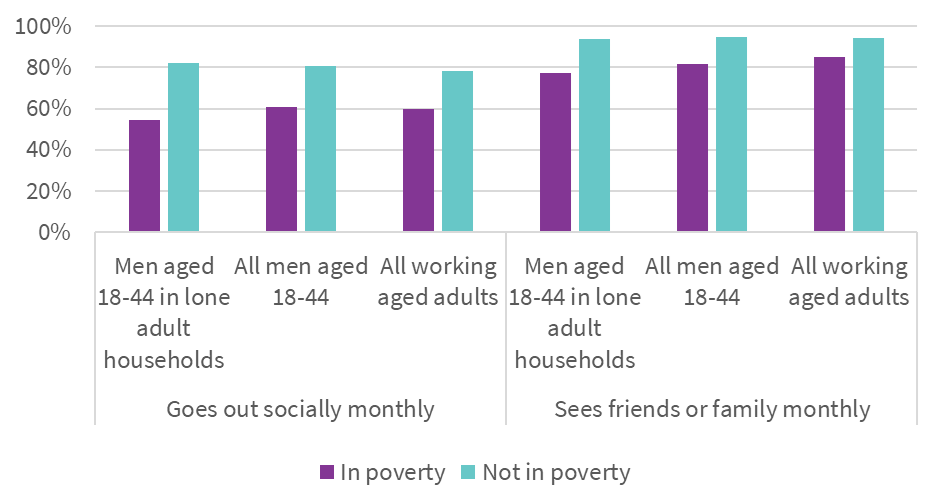
Source: SHERU analysis of DWP (2025) Households Below Average Income (HBAI) (95)
In total, approximately 55,000 men aged 18-44 in Scotland in 2023 said that they did not go out socially and did not see friends or family outside their households monthly. This is important given the emphasis that participants in qualitative research tend to place on friends and family as a source of support:
“I can say my friends were the ones who gave me hope…so, it was actually them who came and just knocked at my door and they are the ones who got me out of my house… I think if I had stayed in the house for much longer, maybe I would have succeeded in, you know, taking my own life. But I’m really grateful for them. They took me out and they bought me food, they bought me drinks, and I was really happy. They even brought me back home. So, yeah, I really appreciate them. And they showed me another side of life, even though I had lost hope in everything. I really appreciate them. Even though I’ve never told them about what I was…I did before, but it was really…it really changed my mood and how I felt about myself. And I can say it was…maybe they were my angels, you know. I don’t know, but I’m really glad for them. If it were not for them, I don’t think I would be around.”
Lewis (149)
Recent research highlights the need for more tailored support for young men. A co-produced study with justice-experienced, LGBTQ+, and asylum-seeking or migrant young men in Scotland found that a lack of compassionate support undermined trust in services and underscored the need to normalise conversations about mental health:
“The circles we kicked aboot with, no[one] talked about mental health, so we didn’t think about mental health, you didn’t realise your mental health was shite, you just thought you were normal.”
Mack (115)
Similarly, a recent report exploring the impact of employment and financial instability on suicidal thinking and behaviour in Scotland highlights participants’ sense that limited public sector support is available:
“It feels like the world is falling on your head and there is no solution to it. And no one is trying to reach out and trying to…even the Government is not doing anything. Nobody is trying to, you know, find a solution. You just keep sinking deeper and deeper and there is no hand to cry or no shoulder to cry on. I feel lost inside.”
Lewis (149)
[1] This figure excludes men who are inactive due to education or early retirement.
[2] Priority families include lone parent families, minority ethnic families, families with a disabled adult or child, families with a younger mother (under 25), families with a child under 1, and larger families (3+ children).
[3] Excluding white minorities
Interim adverse outcomes and possible early intervention points: homelessness and interactions with the justice system
Homelessness is directly bound up with deaths due to drugs, alcohol or suicide, and single men are most likely to be homeless.
In 2023, 57% of all deaths among homeless people were due to drugs, alcohol, or suicide – compared to 19% of all avoidable deaths (110) (and 5% of all deaths) among the population in general (150). Men accounted for 79% of all deaths among homeless people, and men aged 15-44 specifically accounted for 40% of all deaths among the homeless population. The average age of death among men experiencing homelessness was 46 years old (60). A retrospective cohort study that linked administrative data found that premature death in Scotland was significantly higher among people who experienced co-occurring homelessness, justice involvement and/or opioid dependence (151).
Homelessness applications in general have risen substantially over time in Scotland. Single male households are the most likely group to experience homelessness, accounting for 49% of all homelessness applications in 2024-25.[1]
Figure 6.13 Number of homelessness applications made by men
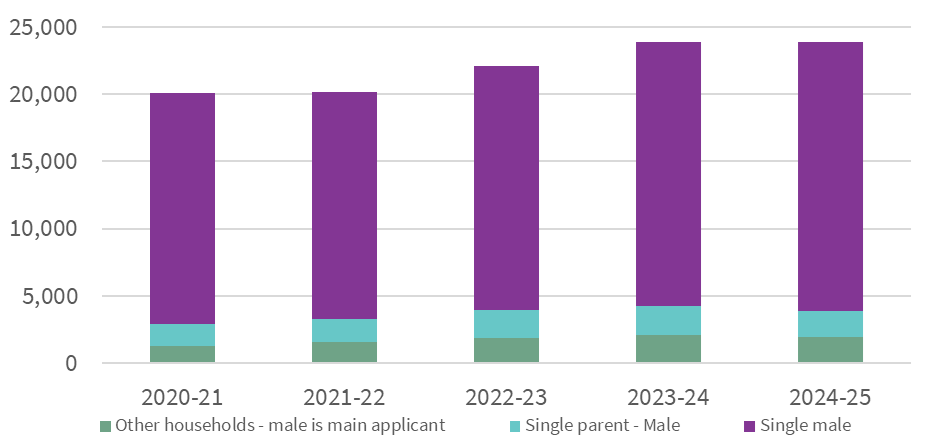
Source: Scottish Government (2025) (90)
Single male households were also more likely to experience rough sleeping compared to others. Of the 40,690 homelessness applications made in 2024-25, 3,580 had experienced rough sleeping at some point in the three months prior to making an application. Of these, 2,760 were single men.
While rough sleeping only accounts for a sub-set of homelessness, it comes with very serious health risks, including exposure to harsh weather and violence, a lack of access to healthcare and a higher likelihood of untreated medical conditions (152–154). There have been attempts to support the healthcare needs of homeless populations in Scotland’s three largest cities – Edinburgh, Glasgow and Aberdeen – through specialised GP practices (an example that cuts across secondary and tertiary prevention). However, in March 2023, a decision was taken to close the dedicated GP practice for people experiencing homelessness in Glasgow. In 2025, a report from the Independent National Whistleblowing Office criticised this decision, noting the failure to properly assess the likely impacts of this decision on health outcomes, including the impact on emergency departments in hospitals (155).
In Scottish research, people in this situation describe life on the streets as fraught with physical danger and societal stigma, which informs a sense of inescapability:
“I call it [the street] the devil’s playground – the folk living rough, you become part of it, and you don’t get a chance to change. Everyone on the street, like us, and they have no chance to change their lives. It’s like a black hole”
Dave (156)
There are further challenges for people from ethnic minority backgrounds. Whilst people from ethnic minorities represent around 13% of all homelessness applications – a proportion roughly comparable to their overall proportion of the Scottish population – they may experience different challenges navigating the housing system.
“You have to bid for online, and that disadvantages anybody who’s no good at … English language, doing online, or who’s poor at using computers … It’s an unfair system, which is basically a system of housing rationing … The presumed colour blindness of the system, and the presumed, ‘Oh we’re not discriminating’, when in fact the system is extraordinarily discriminating”
Ian, Resident, Glasgow(157)
Evidence from research on interactions with the justice system point to issues with support provided at this critical intersection
Scotland’s incarceration rate is substantially higher than that of most European countries (158), and many men cycle in and out of prison across adulthood. In 2023-24, men made up 96% of the average daily prison population, and 64% of prisoners were aged 25–44.
The prison population has been aging noticeably in the past 15 years, with the number of adults aged 18-29 in prison declining by 51%, while the prison population for adults between the age of 30 and 44 has grown by around 33% (Figure 6.14). This is partly because there are more people serving longer sentences for more serious crimes (159)
Since 2019, the justice system in Scotland has made a presumption against short prison sentences of 12 months or less and has aimed to shift cases to community sentences where possible (160). In 2024–25, Scottish ministers also changed release rules for short-term prisoners (those with sentences under four years) so that most are now automatically released after 40% of their sentence has been served, with the aim of reducing Scotland’s high prison population (161). It is not yet clear how this might be impacting socio-economic or health outcomes for relevant populations and it would be good to see research aiming to assess these impacts.
Figure 6.14 Average number of adults in prison by age band
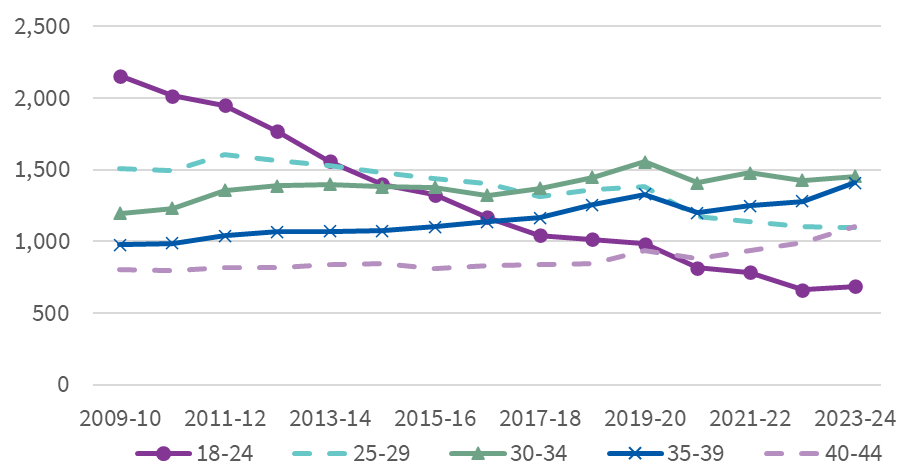
Source: Scottish Government (2024) (162)
Imprisonment is also closely tied to drug use and access. Participants in a recent qualitative study exploring the intersection of drug addiction and mental ill health among men in Scottish prisons included multiple accounts of how easily available ‘legal’ drugs were contributing to worsening mental health, paranoia, and violence in prison:
“It’s just all ‘legals’ now [in the jail]. It’s destroyed the jail, all the good people. It’s made them mentally insane n’that … just made everyone paranoid. You canny trust anyone. My pal attacked me on Christmas morning with a snooker cue … for nothin’, he was just pure paranoid.”
Joel, age 23 (163)
“That legal stuff people are takin’ … you see people gettin’ freaked out with it … the jail’s ruined with it … you could turn your back for two minutes and someone could hit you and they don’t even know they’re dain it so you don’t know what to expect. It’s dangerous stuff … it’s like chemicals on a bit of paper.”
Ben, age 29(163)
The period after release from prison is often especially chaotic and risky. An older data-linkage study found that drug related mortality for men was seven times higher in the two weeks following release than at other times of liberty and 2.8 times higher than prison suicides (164).
A recent, small-scale study that involved interviewing five men who had experienced time in Scottish prisons about their experience of re-entering society on release found that social isolation, a sense of stigmatisation and poor mental health were common features:
“It’s great depression, you know, to be judged, before they even meet you. I spent so many years sitting in a room. You know, that’s the main part of the major depression, you know? (…) I pretty much gave up at one point. So it almost felt like I was in prison and myself and one bedroom.”
Participant (165)
“You’re trying your best, and then, you know, it’s always the thing when you think, well, what’s the point? What’s the point of, like, trying to live a normal life? Because you’re trying really hard to, like, not take drugs, and you’re trying really hard, you know, not to, like, commit crimes to get money, but the world is putting up all these barriers in front of you.”
Participant (165)
People released from prison have high likelihoods of reoffending as well, with young adults being the most likely to reoffend. This has decreased over time, but cycles of incarceration and convictions remain a concern. A longstanding pattern persists, with males experiencing higher reconviction rates than females. Among all offenders in 2021–22 whose most recent offence was drug-related, 26.4% had 1–2 prior drug convictions and 7.3% had 3–10, highlighting the link between cycles of imprisonment and drug use.
Figure 6.15 Proportion of offenders who were reconvicted within a follow up period of one year
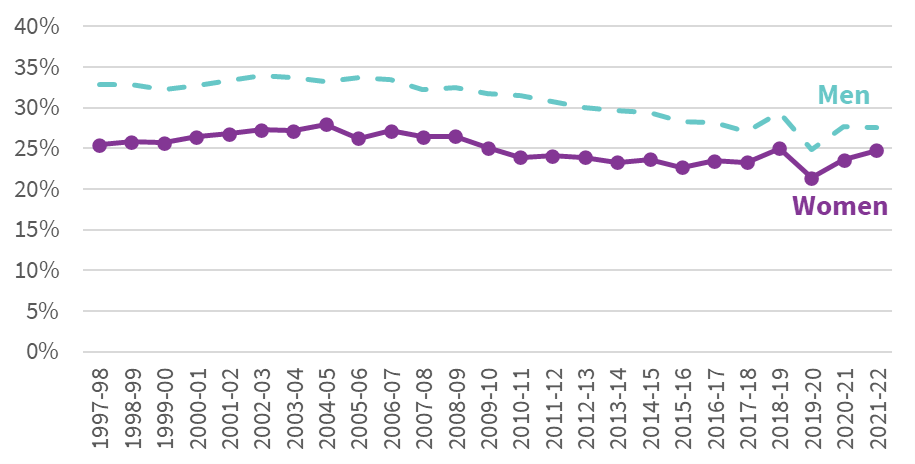
Source: Scottish Government (2025) (166)
National mapping shows that most prison mental-health teams include psychiatry and psychology but that these services are so overstretched that they are often only able to provide an emergency service, leaving the majority of the prison population with no routine support (167).
[1] Men in general accounted for 59% of all homelessness applications in 2024/25
Exploring examples of prevention and joined-up governance to tackle socio-economic determinants to improve health outcomes and lessons for Scotland
Published in 2011, the Christie Commission on the Future Delivery of Public Services calls for a joined-up policy approach to prevent poor health outcomes in the long run, but in the years since its publication, progress has been slow (168). Despite repeated efforts to facilitate “whole of government” responses to Scotland’s poor health outcomes, the Scottish Government has struggled to implement cross-government initiatives that tackle socio-economic inequalities with the explicit purpose of improving health.
By cross-government, we are referring to collaboration across Scottish Government directorates (horizontal collaboration) as well as with delivery partners (vertical collaboration). As we will see later in this chapter, there is a significant amount of partnership and collaboration expected at the local (vertical) level to deliver programmes, however, concerns remain about the extent of genuine integration within the Scottish Government’s structure.
The Scottish Government, as is the case with many executive bodies, is split into a structure that aligns to Ministerial portfolios. For example, civil servants who work on health inequalities sit under the Cabinet Secretary for Health and Social Care and civil servants who work on housing sit under the Cabinet Secretary for Housing. Budgets are allocated along similar lines. Cabinet Secretaries, or junior Ministers, are held to account for the delivery of strategies and action plans aligned to their policy area based on the levers (and budgets) held within their directorates.
This should not make it impossible to design joined-up policy, and indeed the Scottish Government’s National Performance Framework was meant to act as a catalyst to ensure all were working to the same aligned outcomes. However, from 2008’s Equally Well: Report of the Ministerial Task Force on Health Inequalities (169) to the more recent Population Health Framework (170), we have seen a consistent pattern in which impressively cohesive, evidence-based analyses of the factors that shape population health are not matched with joined-up policy plans for shared actions, or shared budgets.
As a result, the government and the public services it supports are struggling to realise rhetorical commitments to prevention or to improve key social determinants of health, such as housing, by joining up priorities and budgets across directorates (171). Engagement with those involved in service delivery have told us that the siloed nature of Scottish Government directorates is constraining their efforts to effectively deliver services that meet the needs of the communities they serve. This was also a key finding of work Nesta took forward with a range of stakeholders across Scotland for Health Foundation’s Leave No One Behind Report (2).
Against this backdrop, we want to showcase two examples in which other countries have successfully implemented joined-up approaches to preventing poor health outcomes where central government has had a clear enabling role. Informed by a SHERU webinar in June 2025 (172), we explore:
- An Irish approach to developing a cross-government, cross-sector infrastructure to support the implementation of their suicide prevention strategy, Connecting for Life, in place from 2015-2024.
- The Icelandic prevention model, which focuses on young people, and which has been developed from 1997 onwards.
For each case, we briefly summarise the actions that have been taken and the evidence to date exploring impacts on health and health inequalities, before closing with some reflections on what the key takeaways for strengthening prevention work in Scotland might be.
Ireland: Infrastructure to support the effective implementation of a suicide prevention strategy
Ireland’s suicide prevention strategy is a unique example of an effort to address the infrastructural challenge of joined-up working. Its most recent strategy focused on social, economic, and spatial policies to reach the communities most likely to be affected by inequalities, and most at-risk of suicidal behaviour.
The Connecting for Life strategy was in place from 2015-2024. It is now at the evaluation stage (173). It follows from earlier strategies, starting with decriminalisation of suicide in 1993, the establishment of the National Task Force on Suicide, which operated from 1995 to 1998, and Reach Out, Ireland’s national strategy from 2005-2014 (174). Connecting for Life sought to improve public awareness, reduce access to means of suicidal behaviour, and to improve care pathways and broader support services for people vulnerable to suicide.
The strategy also considered the upstream preventative factors discussed in the previous chapter, such as housing, employment, education, and social capital, and established a governance mechanism to ensure an ongoing focus on implementing action across these areas: a National Cross-Sectoral Steering and Implementation Group. This group is charged with driving policy implementation and change. It is chaired by a senior official in the Department of Health but there are representatives from a wide range of departments, enabling peer-to-peer questioning, consideration and discussion across different departments, with a focus on tracking progress, with delivery and implementation. Local Authorities and third sector organisations are also represented on the group, facilitating vertical connectivity (from community to government) alongside horizontal (within central government) working. This group reports to a Cabinet Sub-committee, which further reviews progress with delivery and implementation. In reflecting on the Irish government’s architecture to support the delivery of their suicide prevention strategy during the SHERU webinar, Professor Steve Platt noted that:
“In over 40 other national suicide prevention programmes, I don’t know of any other that has this kind of mechanism for actually attempting to deliver a whole of government policy.”
Professor Steve Platt (172)
Alongside this, the Irish National Office for Suicide Prevention (NOSP) encouraged other departments to consider how suicide prevention is built into their work. These departments include Rural and Community Development, Children & Youth, Health, Mental Health, Social Protection, Justice, Defence, and Employment Affairs (175). The NOSP also worked with local areas to implement suicide prevention strategies relevant to local needs and capacity.
We need to wait for the evaluation to understand to what extent these changes can be attributed to the implementation of the strategy. We do not have directly comparable data for Scotland on suicide, with Scottish data also including deaths of “undetermined intent”. However, we can see that during the Connecting for Life strategy, rates of suicide where death was denoted as being intentional self-harm in Ireland diverged noticeably from the Scottish figures for intentional and probable suicides (Figure 6.16).
Figure 6.16 Male suicide rates per 100,000 population in Ireland and Scotland, indexed to 2000
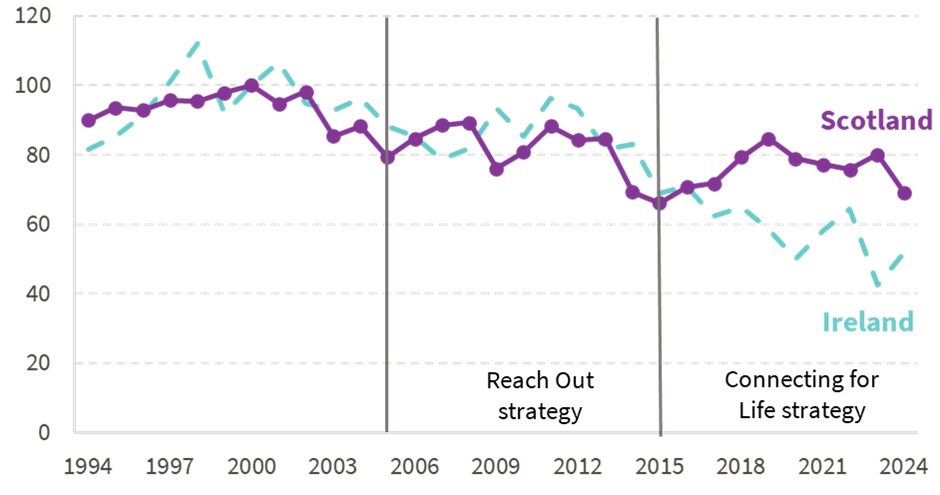
Source: Central Statistics Office (176), NRS (99)
Note: Republic of Ireland data lists the cause of death as intentional self-harm (ICD-10 code: X60-X84). Scottish data also includes Events of undetermined intent (Y10-34), Sequelae of intentional self-harm (Y87.0) and Sequelae of events of undetermined intent (Y87.2)
Iceland: Preventing alcohol and drug harms in young people
While Ireland’s suicide prevention model is embedded across varying levels of government, the initiatives, oversight, and planning are centralised at the highest level. Iceland’s model for preventing harmful drug and alcohol use among young people is set up rather differently: while it was steered and developed at the top level, it is organised and implemented almost entirely locally.
The Icelandic Prevention Model began in 1997, in response to a rise in adolescent alcohol, drug, and tobacco use (177). Early studies (177,178), sponsored by the government of Iceland and the Reykjavik City Council, identified four key factors that are likely to influence adolescent substance use:
- Peer groups
- Schools
- Families
- Leisure time
The researchers noted that their findings suggested different communities would need different types of support. In response, the government worked with others to develop a community-based, collaborative approach that aimed to address the root causes of harmful substance use among young people.
The resulting model involves a broad, central government ten-step framework, accompanied by funding, which requires coalitions of local actors to agree what actions they will take to help achieve collaborative goals across these four areas annually, and to implement the relevant approaches within their own communities. These goals are informed by an annual survey of primary and secondary students, where they are asked about substance use and their perceptions of the four areas identified above. The related strategies may be policy-based, implemented with the help of third sector organisations, or achieved through community outreach. The survey is also used to assess progress and understand the efficacy of previous initiatives (179).
Although the Icelandic model is intentionally designed to enable different local areas to make contrasting decisions about how best to prevent the harms caused by alcohol and drugs amongst local communities of young people, central government plays an important role in four key ways. First, it provides a clear framework that specifies the four factors that local areas should consider. Second, it supports key data insights through the annual survey of young people, to inform local understanding and decision-making. Third, it provides multiple resources. This includes direct funding to adolescents for leisure time activities via a recreational voucher, equivalent to around £500 annually, that can be used towards recreational programmes or activities. It also includes grant funding to third sector organisations lasting a minimum of five years (180). This change did not necessarily increase the amount of expenditure on these programmes; rather, it restructured the timelines and distribution of financing (179). Finally, a centralised body, The Icelandic Centre for Social Research & Analysis (ICSRA), provides central oversight for the programme, by administering the survey annually, overseeing trends, providing advice for local communities, and evaluating the efficacy of various strategies.
Joined-up working in Scotland – vertical vs horizontal
In looking for examples of joined-up working in Scotland, we were struck by the range of programmes and approaches that are there to ensure person-centred and joined-up approaches in Scotland within the delivery landscape that are relevant to tackling the socio-economic determinants of health.
Examples include:
· The Whole Family Wellbeing Funding approach which is seen as central to delivery of The Promise in Scotland. This approach uses Children’s Services Planning Partnerships (CSPPs), that operate within a local authority area, bringing together the local authority, NHS Board, Police Scotland, third sector organisations, and other partners including representatives from housing, justice and other relevant local services. This approach is underpinned by the Children and Young People (Scotland) Act 2014 which made joint children’s services planning a statutory requirement.
- The Community Link Workers programme embeds non-clinical staff in GP practices in deprived areas, to help patients address social determinants of health such as housing, debt, benefits, loneliness, and community connection (181). An early version was first piloted in Fife and Glasgow from 2010-2011, with support from the Scottish Government. The insights informed the randomised roll out across seven Deep End Links Worker sites in Glasgow in 2014, and the Health and Social Care Alliance Scotland (the ALLIANCE) oversaw an evaluation of the project (182). In 2016, the Scottish Government committed to funding 250 Community Link Workers across Scotland (183). Funding comes from the Primary Care Improvement Fund within the health directorate.
- Alcohol and Drug Partnerships (ADPs) are the primary local delivery mechanism for the National Mission on Drug Deaths (184). ADP membership includes the local authority, NHS board, integration authority (IA), Police Scotland, Scottish Prison Service, third sector organisations and community members. One of the main findings of a recent Audit Scotland report noted that more joining-up is required among partners in health, social care, education, housing, prison, and community justice settings, and ADPs themselves have said they would like a stronger focus on the role that other services can play and more focus on prevention (185).
- Local Employability Partnerships (LEPs) deliver No one Left Behind, Scotland’s approach to employability support. Every local authority area in Scotland has an LEP, reporting into Community Planning Partnerships (itself a joined-up delivery body), with membership including Local Authority employability leads, Skills Development Scotland, DWP/Jobcentre Plus, Further and Higher Education, Third Sector Interfaces, specialist service providers and representatives of service users (186).
These examples show that the principle of joined-up working is integral to how the Scottish Government sets expectations for the delivery of some programmes, sometimes to the extent of embedding the approach in statute. This report is not the place to review the effectiveness of these approaches in detail, but we are particularly interested in how the Scottish Government supports these delivery mechanisms; the Irish and Icelandic examples make it clear that central government was a key part of making their interventions.
In speaking to stakeholders involved directly or indirectly in delivery of these programmes, a common theme has emerged: the collaboration at local level is not mirrored at Scottish Government level. For example, there does not appear to be formal joint governance arrangements across relevant portfolios. Relatedly, we have not come across approaches to share budgets across portfolios to meet outcomes, which leaves programmes vulnerable to decisions made within single portfolios. Audit Scotland have noted this with respect to Community Link Workers, where a 2021 decision was made to prioritise spending from the Primary Care Improvement Fund on three other services, leaving Community Link Workers insecure and vulnerable to the short-term nature of the funding left available to them (187).
There is also reference made in published reports to a lack of routine sharing of data and information from these programmes across different parts of government, leading to organisations being asked for the same information multiple times depending on their membership of different delivery partnerships. Interviews carried out by PHS with ADP leads showed frustration with coordination at the national level in relation to the National Mission on Drug Deaths, for which ADPs are a key delivery partner. Only a quarter (23%) of respondents agreed that there was good coordination between the different national organisations and teams involved in the National Mission on Drug Deaths (185).
Partnership working was also examined during the post-legislative scrutiny of the Community Empowerment (Scotland) Act 2015 which strengthened the role of Community Planning Partnerships (who incidentally are a key part of the delivery mechanism for the Population Health Framework published in June 2025).
A comment from one of the evidence sessions captures the challenge we have observed particularly well:
“Clearly, community planning is about an integration model, but there is no homogeneous model across the whole public sector in Scotland with regard to policy making. That remains a key driver for what happens in many of the public bodies and partners that you talked about.
We exist in silos that are, ultimately, driven by a policy system that is linked to Government and to a particular cabinet secretary. That is the tram line that bodies are set on, but they are asked, at the same time, to integrate and work in partnership with others.”
Mark McAteer, representing the Community Planning Improvement Board (188)
While published reports provide some insights, much of the concern about how the Scottish Government supports joined-up working has emerged through informal, off-the-record, conversations. There is comparatively little research that examines this issue directly. A number of factors may explain this. For instance, because the Scottish Government often commissions or funds evaluations, these studies tend to focus on how funded organisations collaborate, rather than on how government itself operates. In addition, organisations that rely on Scottish Government funding may be reluctant to put their concerns on record for fear of jeopardising their relationship (and future funding).
We hope to be able to add insight into this as part of our Supporting Policy Implementation workstream, which is working with local authorities and some of their partners to explore how national policy is delivered in housing and employability. We hope to publish our first set of reports from this workstream this later this year.
What insights might help Scotland prevent deaths from drugs, alcohol and suicide?
Given the extent to which men are dying from drugs, alcohol, suicide, and related conditions, and knowing that two small, nearby countries have developed – and had success with – cross-governmental, joined-up approaches to preventing these outcomes, what are the potential insights for Scotland in efforts to reduce such deaths?
The Scottish Government has strategies covering suicide prevention (published 2022) (189), alcohol harm (published 2018) (190), as well as the National Mission on Drug Deaths (published 2022) (191). Much like the recent Population Health Framework, all these strategies reference the need for a cross-government approach to tackle the issues but do not set out how this will be achieved in practice.
The strategies all highlight the high death rates for men, yet there is little discussion of what needs to happen to focus upstream prevention on younger adult men, or what such prevention measures might involve. For example, in the National Mission on Drug Deaths, Outcome 5 is framed around improving services such as housing, welfare and income needs for users of drugs, but does not make similar references to the support being required earlier to help prevent problem drug use. Outcome 1: “Fewer people develop problem drug use” has references to the government’s wider commitment on addressing inequalities and the social economic determinants of health but does not provide specific actions as to how this strategy will lead to the change required.
As we have set out, we think there is a policy blind spot when considering socio-economic policy focused on men aged 18-44. That is, across government, there does not seem to be the recognition that younger adult men need additional support. This is partly due to a lack of visibility of the issues at this life stage because, on average, men in this age group do well economically compared to other age and sex cohorts. This can mask the issues that a subset of men face. Government strategies on suicide prevention, alcohol harm and drug deaths all talk about interconnectedness across different aspects of policy but this does not seem to be recognised in how policy is developed outwith these strategies and across other parts of government. Our analysis has shown that potentially at-risk men often have experiences of imprisonment, homelessness, poor quality work or no work at all, low or no qualifications, growing issues with poverty and social security, health crises, social exclusion and isolation. More likely, they have experiences that cross many, if not all, of these domains.
Reflecting on these two international examples from Iceland and Ireland and exploring Scottish examples of local delivery, our sense is that Scottish Government efforts to reduce deaths from substance use and suicide require at least two developments:
First, improvements in our understanding of at-risk individuals through mixed methods (quantitative and qualitative) research exploring the experiences and trajectories of young adult men, with a focus on potential points of intervention, mapped to current policy priorities and to local areas. This intelligence needs to be shared with those who can make use of this evidence in designing policies and tailoring implementation.
More effective, cross-sector governance and budget arrangements to support the implementation, delivery and ongoing evaluation of key existing programmes. The scheduled review of the National Performance Framework at the start of the next parliamentary session provides an opportunity to revisit the original purpose of outcomes as a means to drive policy. Before that, the Spending Review this autumn could be used to set a new approach to how budgets are operationalised for realising cross-government priorities.
These are explored and expanded on in our overall recommendations and conclusions.