Poverty, Prevention, and Fairness
View the report as a PDF here.
Introduction
Scotland experiences some of the largest health inequalities in Western Europe. Life expectancy differs by more than a decade for people living in the most and least deprived areas of Scotland, and the gaps in healthy life expectancy are even larger, meaning that people in more deprived communities spend substantially more of their lives in poor health before death (1,2). These inequalities have persisted over time, with evidence of stalled or limited progress since the early 2010s and continuing challenges linked to preventable ill health and wider social and economic disadvantage (1,3).
Public understandings of health inequalities are an important part of the evidence base when designing new policies, strategies, or programmes. Even the most promising evidence-based policy proposals may be deemed politically unfeasible if policymakers believe public opinion is opposed (4). Indeed, a concern that there may be a limited public mandate for the kinds of proposals that researchers suggest are required to reduce health inequalities has been identified as an important barrier to more effective policies (5,6).
With this in mind, SHERU funded 11 questions in the Scottish Social Attitudes Survey, to get a sense of how people in Scotland understand health inequalities, what they think about the social and structural conditions that shape health, and what they believe should be done to address these issues. These 11 questions broadly cover four domains: health inequalities (causes and desire for action); Scotland’s attempt to take more preventative approaches to policy; which options for improving key social determinants of health (employment and housing) people think are most likely to be effective; which options for reducing deaths from drugs, alcohol, and suicide people prioritise; and experiences of fair treatment by public services and employers.
We looked at how different groups understand these questions, finding notable differences between men and women and people living in deprived and non-deprived areas. We also found some interesting differences comparing the general Scottish population, who are largely white, urban, and over age 44, to people from minority ethnic backgrounds, young adults, and people living in rural or remote parts of Scotland.
Methods
The data discussed in this report was collected on the Scottish Social Attitudes survey (SSAS) in 2025 via a web survey. Letters were sent to a random sample of addresses inviting up to two people per household to complete the survey online, with an option to be interviewed by phone if preferred. The same approach was used in the 2023 and 2024 versions of the SSAS. A detailed overview of the survey design, response rate, and fieldwork is provided in Annex 2. Our analysis explores 11 questions across a range of socioeconomic strata, using calibration weights provided by the SSAS. Examined variables and the non-weighted number of respondents are provided in Annex 1.
Headline insights
Public concern about health inequalities in Scotland is very high, with overwhelming agreement that government action to reduce the health gap between richer and poorer groups is important (94% of people in Scotland said it was either quite or very important).
Although many people (47%) focus on smoking, alcohol, and diet when asked to identify the main cause of health inequalities in Scotland, responses show that people recognise the social and structural drivers of poor health, including poor housing. There are also notable differences between people in the most deprived 20% of areas, who are more likely to cite smoking, alcohol, or stress, and people living in the least deprived 20% of areas, who are more likely to identify diet as the main explanation.
Public views on the most effective options for addressing Scotland’s housing shortage, housing quality, and employment are split across multiple options, which suggests that the Scottish public support multi-faceted approaches.
Deaths from drugs and alcohol are primarily seen as a social problem, with poverty reduction identified as the most effective response to reducing deaths from drugs and alcohol (24% of the public chose this option). Support for punitive policy responses to drugs and alcohol in Scotland is extremely limited (only 1% of the public chose the option “tougher laws/sentencing/enforcement” and hardly anyone chose “control/restrict benefits” as an option).
Investing in mental health services was by far the most popular option for reducing deaths from suicide in Scotland (53% of the public chose this option), with reducing poverty the second choice (16% chose this option). People who identify as being part of minority ethnic communities in Scotland place greater emphasis on education as a means of reducing deaths from drugs, alcohol and suicide.
Support for prevention is strong but conditional: most people favour balancing preventative policies and practices with responding once issues have arisen (for health and housing), but people from the 20% most deprived areas are more cautious about shifting resources away from crisis support.
Most people report fair treatment by public services, but experiences of unfairness are socially patterned. Reported experiences of unfair treatment did not always align with patterns identified in existing research. Some groups reported lower levels of unfair treatment in their current/last job than expected, particularly people from minority ethnic backgrounds.
People living in the 20% most deprived areas in Scotland often gave notably different answers. This suggests that people living at the sharp end of inequalities hold distinct views about priority areas of policy action and about which policy options are likely to be most effective.
What do people in Scotland think causes health inequalities?
Previous research suggests that most people in Scotland are aware that health inequalities exist and view them as an important social issue. Qualitative and survey-based studies conducted over the past two decades in the UK consistently find high levels of recognition that people living in more disadvantaged circumstances experience poorer health (7–9). There is also some evidence that awareness of health inequalities has become more widespread during the period of post-2010 austerity and, more recently, during and after the COVID-19 pandemic, as inequalities have become more visible in public discourse and everyday experiences (10,11). However, while awareness of health inequalities appears relatively high, research exploring what people in Scotland believe causes these inequalities paints a more mixed picture.
For example, studies differ in the extent to which they find people emphasising behaviours (such as smoking, diet, and alcohol use) and referring to wider social and structural determinants (such as poverty, housing, work, and access to services). Research conducted in Scotland and the wider UK has, over several decades, consistently found that behavioural and individualistic explanations are prominent when people are asked for their immediate thoughts on the causes of health inequalities (11–13). In contrast, a review of multiple qualitative studies conducted in Scotland reveal more complex, multi-layered accounts, in which behaviours are understood to be shaped by material conditions, place and stress (14). Some UK studies have found that people living in more disadvantaged circumstances are more likely to articulate structural explanations of health inequalities than those in more advantaged positions, with authors suggesting that this is likely to reflect variations in individual lived experiences (15,16).
What the Scottish Social Attitudes Survey found
When asked to identify the main reason for poorer health among people who are less well-off, just under half of the Scottish population emphasised factors that are traditionally thought of as “lifestyle” factors. Overall, 47% of people felt that poorer health was related to diet, smoking, or alcohol use.
However, there were notable differences between population groups. People from minoritised ethnic backgrounds were much less likely to cite diet as a key explanation and were more likely to emphasise smoking and drinking, housing quality, and access to healthcare.
Similar patterns were evident by area deprivation. Among people living in the most deprived 20% of areas, smoking, drinking, and stress were the most commonly cited explanations, while eating well was less frequently emphasised. By contrast, people living in the least deprived areas were less likely to cite smoking, drinking, and stress, but were around ten percentage points more likely to identify diet as the main explanation.
Urban and rural gaps are also evident. Both urban and rural people were likely to emphasise the effects of diet, smoking, and drinking. However, people in urban communities also commonly cited difficulty accessing healthcare and stress, which were much less common amongst people in rural or remote communities.
Finally, gendered gaps are present: while diet was the most common option for both men and women, women were also likely to highlight healthcare access. Men, especially young adult men or men living by themselves, were much more likely than women to discuss smoking, drinking, and job quality as reasons for health inequality.
These findings mirror existing research in two ways. First, food, alcohol and tobacco, and healthcare, are all popular explanations, aligning with some previous surveys (11,12). Second, there are socially patterned trends within this, showing variation by social group.
However, in splitting key lifestyle factors (namely, by offering “less likely to eat well’’ and ‘‘more likely to smoke or drink’’ as separate options), we found that that people from the most deprived areas were more likely than people from the least deprived areas to focus on smoking and alcohol, and less likely to focus on eating well, while the reverse was true of people from the least deprived areas. Further research is needed to understand the reasons behind this social patterning, though one factor may be inequalities in the availability of tobacco and alcohol and the harms caused by these products (17,18). While the reverse patterning on diet may be linked to a disconnect between research, policy and media concerns about the negative health impacts of obesity and over-eating and the lived realities that increasing numbers of people in more deprived areas of Scotland are facing food insecurity (19).
It is also important to note that, while researchers often interpret public references to the role of alcohol, smoking and diet in health inequalities as evidence that people hold individualistic, behavioural explanations of health inequalities, this is not necessarily the case. Scottish data demonstrate that there are stark inequalities in the harms caused by alcohol (18), smoking (17), and the costs of obesity (20). Research also shows that the marketing and availability of tobacco, alcohol and fast-food products is clustered in the more deprived areas of Scotland (21–23), which highlights the importance of considering how socioeconomic and commercial environments interact. While qualitative research in Scotland shows that, when given an opportunity to respond in more depth, people tend to offer multi-factor explanations of health inequalities that position smoking, alcohol and eating unhealthy food as a response to socioeconomic circumstances (14). This means that, when people identify alcohol, tobacco or diet as a factor in health inequalities, we cannot assume this implies they hold individualistic explanations of health inequalities or that this translates into support for behavioural responses. The fact that “reducing poverty” was the most common response to a separate question asking about the most effective ways of reducing drug deaths in Scotland underlines this point (see p 22).
Chart 1: People in Scotland who are less well-off are more likely to have poor health. Which of the following do you think is the main reason for this?
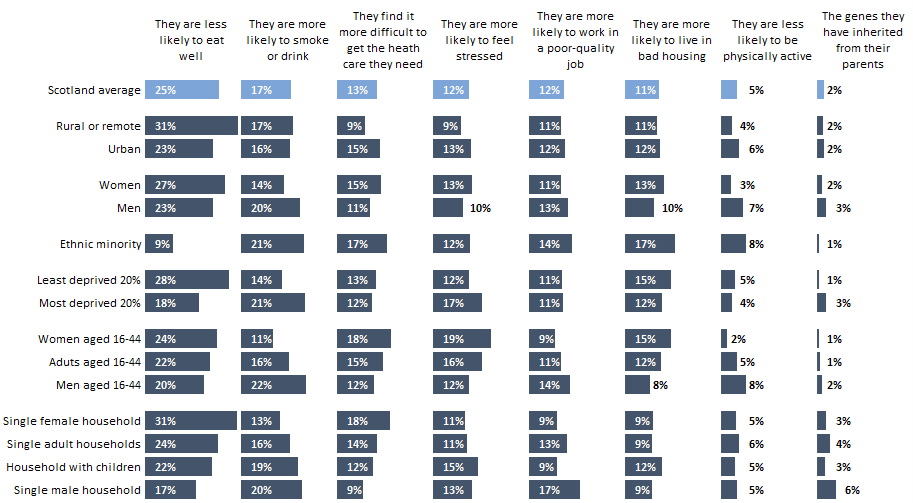
Note: charts exclude “Don’t know” or “Not applicable” responses and may not add to 100%.
How important do people in Scotland think it is to reduce health inequalities?
Previous UK survey data and inequality aversion studies consistently find strong public endorsement of action to reduce health inequalities, including support for government intervention and a willingness to prioritise reducing inequalities even where this involves trade-offs with overall health gains (11,24). Findings using deliberative methods in Scotland reinforce this picture and suggest that support for tackling health inequalities often increases further when people are offered opportunities to engage with evidence and discuss collectively (12,25).
What the Scottish Social Attitudes Survey found
When the Scottish Social Attitudes Survey asked “How important, if at all, do you think it is for the Scottish Government to try and reduce the gap in health between those who are better off and those who are worse off?” 94% of people said it was either quite or very important. This aligns with previous research in demonstrating strong support for policy action to reduce health inequalities in Scotland.
There was limited social variation in response to this question. People from most deprived and ethnic minority groups (e.g., people of “Black, Asian, mixed, or other ethnic origin”) were more likely to say it was important (96%), men and people living in remote or rural areas the least (93%) but the difference between groups was negligible.
Chart 2: How important, if at all, do you think it is for the Scottish Government to try and reduce the gap in health between those who are better and those who are worse off? 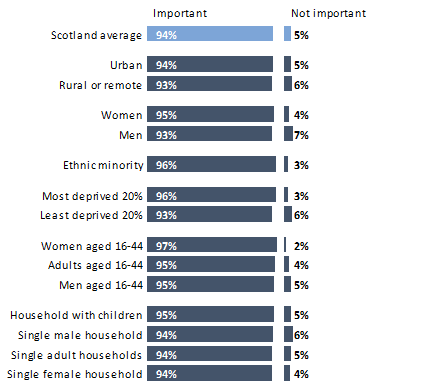
Do people in Scotland support a preventative shift?
Recent Scottish policy has placed increasing emphasis on a preventative shift across public services, seeking to reduce harm and inequality before problems escalate rather than relying primarily on crisis response. This agenda has its origins in the 2011 Christie Commission report, which argued that sustainable improvement in outcomes would require a decisive shift toward prevention, early intervention and tackling the root causes of social problems (26). This approach has been widely cited in Scottish policy documents since 2011 and is reflected in the new Population Health Framework and in Public Health Scotland’s long-term strategy (27,28). Similar principles are evident beyond health, including in housing policy, where recent legislation and reform proposals emphasise preventing homelessness and housing insecurity rather than responding once people are already in crisis (29). However, despite sustained rhetorical and strategic commitment, evidence suggests that delivering a meaningful shift to prevention has proved challenging in practice, with persistent organisational, resource and system pressures and a continuing tendency for services to operate in crisis response mode (30).
Previous UK polling finds strong general support for shifting health systems towards prevention and early intervention, although this reduces somewhat when people are presented with specific trade-offs (11,31). We have not found any survey data exploring public support for prevention specifically in Scotland, despite the strong focus on prevention in recent policy. Against this backdrop, the Scottish Social Attitudes Survey asked respondents to weigh up how the Scottish Government should balance prevention and treatment focused spending for health and housing.
What the Scottish Social Attitudes Survey found
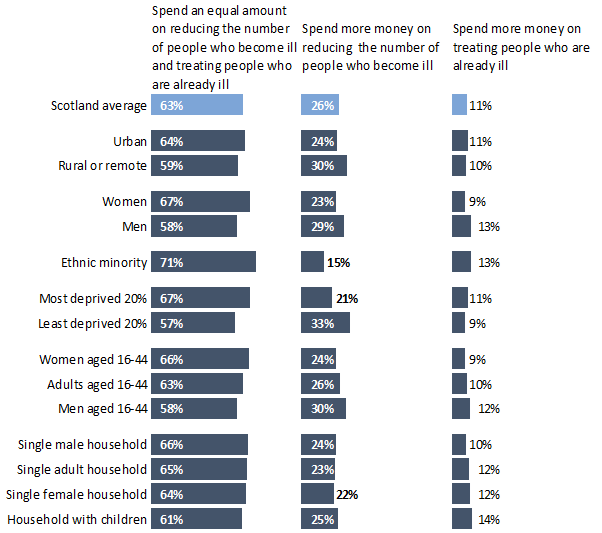
On health, the Scottish Social Attitudes Survey asked: “Suppose the Scottish Government was having to decide whether to spend more money on trying to reduce the number of people who become ill or to spend more money on treating people who are already ill. Which do you think it should choose?”
Here, the data show that majority of people in Scotland support an equal split between the two. Beyond this, the survey suggests more people in Scotland favour prevention over treatment than the reverse, although there were some gaps in the degree to which people favoured even splits or specific directions of spending.
There are also some differences between people from areas of contrasting deprivation, with people from the least deprived areas favouring prevention more strongly compared to people from most deprived regions, who tended to favour an even split. This points to the different experiences facing people at the sharp end of inequalities in Scotland.
There are also notable gaps between women and men; men were more likely to choose to spend money on either treatment or prevention, rather than spending an equal amount on both (though the majority of men – 58% – favoured spending and equal amount on both).
People from minority ethnicities were the most favourable towards an equal split (71% of people who identified as being from a minority ethnic community chose this option).
People from least deprived (33%) and people from remote or rural areas (30%) were the social groups most favourable towards prevention, though the majority of people in both groups favoured an even split.
Overall, the Scottish Social Attitudes survey data align with earlier UK wide data in identifying public support for the current policy focus on achieving a preventative shift; an even split (the most favoured option) would still require a major shift towards prevention since widespread policy rhetoric around prevention has not yet translated into reality (32).
The variations also align with earlier UK wide polling (11,31), though understanding the reasons behind these variations requires further research. It is possible that variations in healthcare needs and access (Such as Scotland’s “inverse care law:” see Bogie et al, 2025 (33)) and variations in people’s ability to pay for treatment privately (34) may help explain why people in least deprived areas were less likely to focus on treatment. In other words, people from the least deprived areas experience less need for health treatment and have more options for accessing treatment when they do need it, all of which might help explain why people in this group were slightly less likely to prioritise spending money on treating people who are already ill. While people at the sharp end of inequalities have greater healthcare needs and often face bigger challenges accessing adequate treatment (33).
Chart 3: Suppose the Scottish Government was having to decide whether to spend more money on trying to reduce the number of people who become ill or to spend more money on treating people who are already ill. Which do you think it should choose?
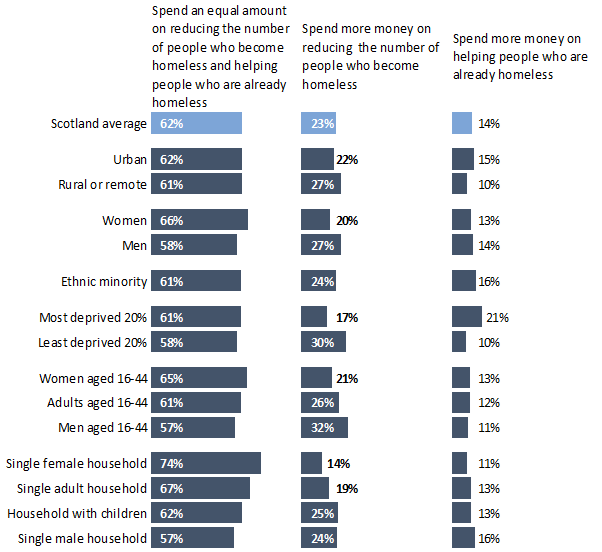
The Scottish Social Attitudes Survey asked a similar question on housing: “Suppose the Scottish Government was having to decide whether to spend more money on trying to reduce the number of people who become homeless or to spend more money on helping people who are already homeless. Which do you think it should choose?”
As with the questions on preventing poor health, the majority of people in Scotland (62%) favoured an even split between prevention and supporting people who are already homeless, with prevention as the second-most popular choice. Further, spending more money on reducing the number of people who become homeless was a more popular choice (23%) than supporting those who are already homeless (14%). One group was an exception to this: people living in the most deprived 20% of areas felt that helping homeless people should receive more money than homelessness prevention, in contrast to people in the least deprived areas.
Women favoured an even split over men, who were again more likely than women to spend more money in one area or the other, rather than both.
As far as we are aware the Scottish Social Attitudes Survey is the first survey that has explicitly asked people to choose between spending more on preventing homelessness versus spending more on helping people who are already homeless. However, separate polling by Crisis in Scotland recently found that 56% of respondents believe the Scottish Government is doing too little to tackle homelessness, with 70% saying political parties should make ending homelessness a national priority (35).
The higher prevalence of homelessness in more deprived areas of Scotland (36) may be a factor in explaining why people from these areas were more likely than those from the least deprived areas to favour spending more money on helping people who are already homeless. However, a fuller understanding of these variations requires collaborative research that can examine how lived experience, local context and structural inequalities shape public attitudes. This aligns with the aims of SHERU’s Collaborative Research for Meaningful Impact, which draws on an Areas of Research Interest approach to strengthen collaboration between research and policy by identifying shared priorities and signalling where new evidence is most needed (37).
Chart 4: Suppose the Scottish Government was having to decide whether to spend more money on trying to reduce the number of people who become homeless or to spend more money on helping people who are already homeless. Which do you think it should choose?
Tacking Major Social Determinants of Health Inequalities in Scotland: Employability, housing and homelessness
Housing and employment are widely recognised as key social determinants of health inequalities in Scotland and the wider UK (38–40), but how people articulate their importance varies by research design and question framing. When people are asked to discuss health in qualitative research, housing frequently emerges as a clear pathway into poor health, impacting both physical health (for example, cold and damp homes worsening respiratory conditions) and mental health (for example, through stress arising from overcrowding, unaffordable rents, and poor neighbourhood conditions) (12,14). Likewise, people’s experience of work, and of being out of work, are frequently cited as important for health, especially mental health, by participants in qualitative research in Scotland) (12,14).
Survey evidence complements this qualitative picture by showing strong public support in Scotland for government action on housing, and widespread concern about job quality, financial security, and work-related wellbeing (41,42). Housing is a particularly salient issue: polling for the Chartered Institute of Housing Scotland shows overwhelming agreement that government should be responsible for ensuring decent housing for all, strong support for rights-based approaches (41), and widespread demand for more affordable homes, while more recent polling by Crisis Scotland indicates that 56% of people believe the Scottish Government is doing too little to tackle homelessness and want greater emphasis on prevention (35).
All this resonates with the current policy context, in which the Scottish Government has declared a national housing emergency, reflecting acute pressures relating to affordability, quality, homelessness and temporary accommodation (29). There is also growing Scottish policy concern about rising levels of economic inactivity driven by long-term sickness and disability, and the implications this has for both health inequalities and labour market participation (43).
Taken together, this evidence suggests that the Scottish public generally sees housing and work as legitimate and urgent areas for government intervention. There has been limited opportunity to assess how people think the Scottish government should intervene on these issues. The latest Scottish Social Attitudes questions help to address this evidence gap.
What the Scottish Social Attitudes Survey found
On employment, the Scottish Social Attitudes Survey asked “The Scottish Government is trying to get people who have not worked for a long time, for example because of sickness, disability, or caring responsibilities, into jobs. Which, if any, of the following do you think would be the most effective way of achieving this?”
People were roughly split between the Scottish Government helping people with disabilities or experiencing ill health return to work and helping employers provide jobs to people with an illness or disability, with childcare also a major concern.
There were some notable differences between men and women, with men favouring growing the economy and women favouring making childcare more accessible. Men were also slightly more likely to favour a benefit reduction compared to the Scottish average (though there was very little support for this option overall).
The roughly even split between supporting people who are ill or have a disability back into work, and doing more to help employers, mirrors the split between preventative and reactive policy options for health and housing. It suggests that people in Scotland believe that these policy challenges require a multi-pronged approach.
Chart 5: The Scottish Government is trying to get people who have not worked for a long time, for example because of sickness, disability, or caring responsibilities, into jobs. Which, if any, of the following do you think would be the most effective way of achieving this?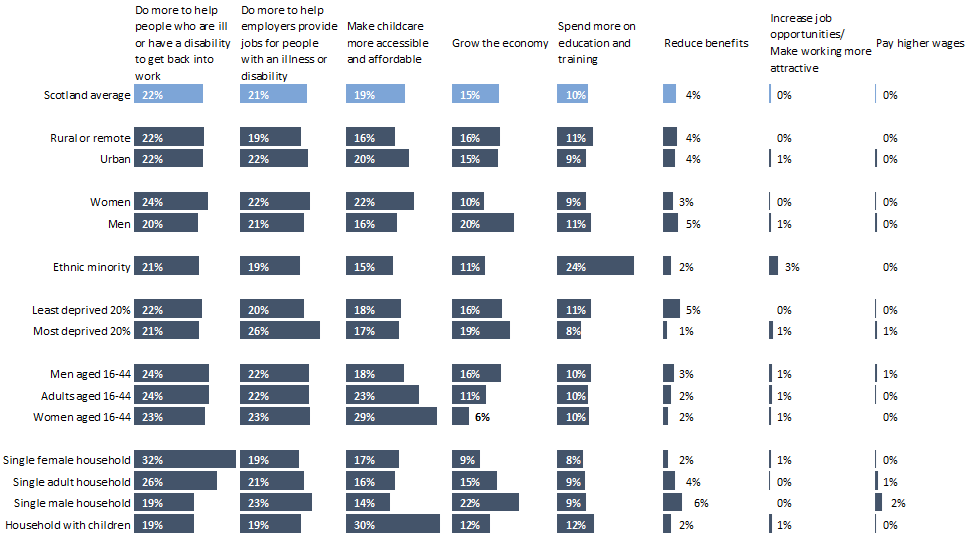
The Scottish Social Attitudes survey also touched on the current national housing emergency, asking “The Scottish Government has said there is a shortage of housing in Scotland. Which of the following do you think is the main reason this has happened?”
Costs were important to people in Scotland, with 37% saying that housebuilders aren’t building houses at affordable prices or that rents are too high. Insufficient social housing was also a big concern, with 21% of people citing this as the reason for a housing shortage.
The findings suggest that people in Scotland do not see migration is a key factor in the current housing crisis is ambiguous. Only 18% of people chose “too many people moving to Scotland” and only 1% of chose “too many houses given to migrants/benefit claimants” as the main reason for Scotland’s housing shortage.
Housing affordability was especially important to adults age 16-44 and people from ethnic minorities, with both groups more likely than average to say that housebuilders don’t build houses at prices people can afford, and that rents are too high.
Social housing expenditure was important to people in non-deprived areas, but interestingly, less so for young adults and people in deprived areas.
Meanwhile, only people in deprived areas felt that too many people are coming to live in Scotland, a sentiment that was not reflected among other groups. This again points to a sense that the lived experiences of people at the sharp end of inequalities in Scotland is markedly different from other groups.
Chart 6: The Scottish Government has said there is a shortage of housing in Scotland. Which of the following do you think is the main reason this has happened?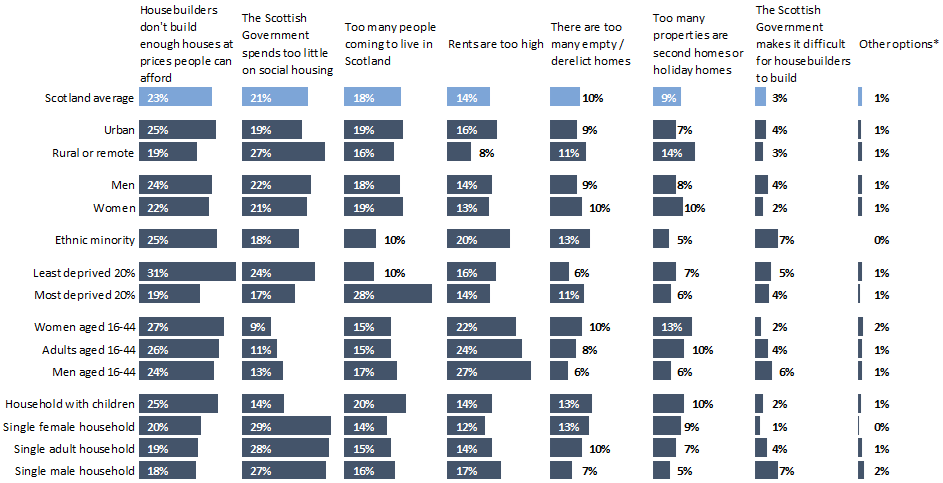
*Other options include: “Too many houses given to migrants/benefit claimants;” “Too many ‘buy to let,’” and “Rents are too low.”
Finally on housing, the Scottish Social Attitudes Survey asked: “The Scottish Government wants to reduce the number of homes in Scotland that are unhealthy for people to live in (e.g. because of damp, mould, cold, etc). Which, if any, of the following do you think would be the most effective way of achieving this?”
People were evenly split about whether investing more in social housing or doing more to enforce housing quality standards was the most effective way to improve unhealthy housing.
Again, people in least deprived areas were the most favourable towards social housing, with 34% citing it as the most effective way to address this.
People from minority backgrounds, young adults, and people in deprived areas again favoured laws to regulate landlords (36%, 26%, and 22% respectively, compared to 19% in Scotland on average). All three groups are more likely than the rest of the population to be living in rented accommodation (social housing or private rented options) and people from minority ethnic backgrounds and young adults are more likely to be living in private rented accommodation (44).
Enforcing quality standards was seen as less likely to be effective by people from minority backgrounds compared to people from minority backgrounds, with only 10% saying that this would be effective compared to Scotland on average at 29%.
Overall, the Scottish Social Attitudes survey results suggest people in Scotland want to see multifaceted responses to the current housing shortage and the problem of poor-quality housing and that investing in building more homes, especially social housing, are priority areas.
Further research is required to explore the reasons behind some of the differences by social group. Greater awareness of long waiting times for social housing (45) could be a factor in explaining why people from the most deprived areas of Scotland are less likely than people from the least deprived areas to see social housing as a solution to poor quality housing. Again, this speaks to the different experiences of those at the sharp end of inequalities.
Chart 7: The Scottish Government wants to reduce the number of homes in Scotland that are unhealthy for people to live in (e.g. because of damp, mould, cold, etc). Which, if any, of the following do you think would be the most effective way of achieving this?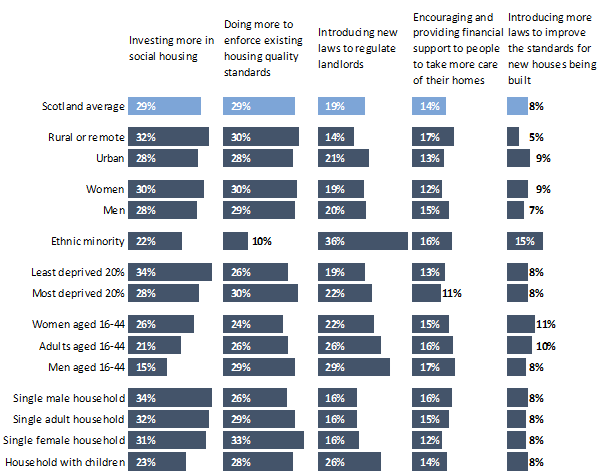
Deaths from drugs, alcohol, and suicide
People living in Scotland experience higher mortality from drugs (46), alcohol (47), and suicide (48) than those in any other part of the United Kingdom. More starkly, Scotland records the highest rate of drug-related deaths in Western Europe and remains among the countries with the highest death rates from alcohol and suicide (49).
As we set out in our 2025 Inequality Landscape report, these harms disproportionately affect men in Scotland. In 2023, males accounted for 70% of deaths related to drugs, alcohol, and suicide. Since 2001, the combined burden of these outcomes has increased steadily, largely reflecting sharp rises in drug-related mortality. Although deaths linked to alcohol and suicide are lower than levels observed around 25 years ago, rates for both have remained largely unchanged over the past decade (2).
Existing qualitative research finds that people in Scotland often describe using drugs and alcohol as ways of “coping” and “escaping” challenging experiences (14). Socioeconomic circumstances (notably poverty and linked sense of hopelessness) are often cited alongside traumatic interpersonal experiences (such as bereavement and abuse) (14,50). While qualitative research on suicide and suicidality in Scotland consistently portrays suicidality as arising from an accumulation of pressures rather than a single cause, with men’s accounts often shaped by relationship loss and bereavement; trauma and adversity (including abuse and long-term exposure to violence or instability); substance use and mental distress; as well as social isolation and difficulty disclosing vulnerability, often linked to norms of masculinity around coping alone and “not talking” (51,52).
The Scottish Government recently published a new, combined strategy for tackling deaths from drugs and alcohol. To this point, however, the National Mission on Drugs and the Alcohol Framework have sat separately, as does the suicide prevention strategy, Creating Hope Together (53,54). The new alcohol and drug strategic plan, Preventing Harm, Promoting Recovery acknowledges the need for early intervention and discusses prevention by providing support to families with young children and through changes to the commercial environment (for instance, by reducing the availability of cheap alcohol through Minimum Unit Pricing and restricting alcohol marketing) (54). The suicide prevention strategy places a strong focus on addressing socioeconomic conditions such as poverty and homelessness, alongside efforts to improve treatment and reduce the stigma of mental ill health (53).
Although socio-economic factors are considered in all three strategies, SHERU has identified a policy “blind spot” in Scotland around support for young, adult men – the population group most at risk of deaths from alcohol, drugs and suicide (2). Much of the broader policy work to reduce poverty and improve housing in Scotland in recent years has not prioritised this population group.
There is limited research exploring what members of the public think about the Scottish Government’s current approach or how they think policy should best respond to deaths from drugs and suicide, though we know a little more about public views on alcohol. For example, a mixed-methods study (combining a nationally representative survey with deliberative group discussion) found public recognition that alcohol-related harm is shaped by structural factors such as marketing, pricing and availability, and identified public support for stronger Scottish Government action on alcohol, particularly regulation of price, promotions and availability (55).
What the Scottish Social Attitudes Survey found
The Scottish Social Attitudes Survey asked: Which of the following, if any, do you think would be the most effective way of reducing deaths in Scotland from drugs and alcohol?
The resulting data suggests people in Scotland see poverty reduction as the most effective way of reducing deaths from drugs and alcohol, followed by an increase in mental health service spending.
There is a notable difference between men and women, with women focusing more on mental health services and less on poverty reduction compared to men and compared to the Scottish average.
People from minority backgrounds have notably different takes from Scotland as a whole, favouring spending on education and on making it more difficult to access drugs and alcohol, while focusing less on poverty and mental health on average. There were limited differences based on area deprivation.
The new survey findings align with existing research identifying poverty as an important factor in deaths from drugs and alcohol (2). Given young, adult men are the group most at risk from these deaths, it suggests a need for policy responses to poverty that go beyond the current Scottish Government focus on reducing child poverty, including for single, adult men who SHERU has identified as currently being a policy “blind spot”(2,56).
The findings also show there is limited public appetite for punitive approaches to drugs and alcohol in Scotland; only 1% of the public chose the option “tougher laws/ sentencing/enforcement” and hardly anyone chose “control/restrict benefits” as an option.
Chart 8: Which of the following, if any, do you think would be the most effective way of reducing deaths in Scotland from drugs and alcohol?
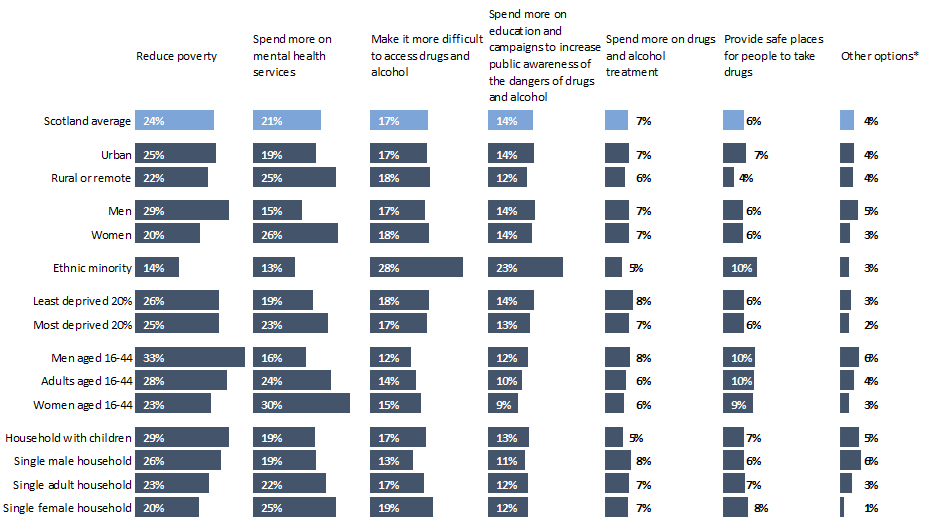
*Other options include: “More research,” “Tougher laws/sentencing/enforcement,” “Decriminalisation/legalisation,” and “Control/restrict benefits”
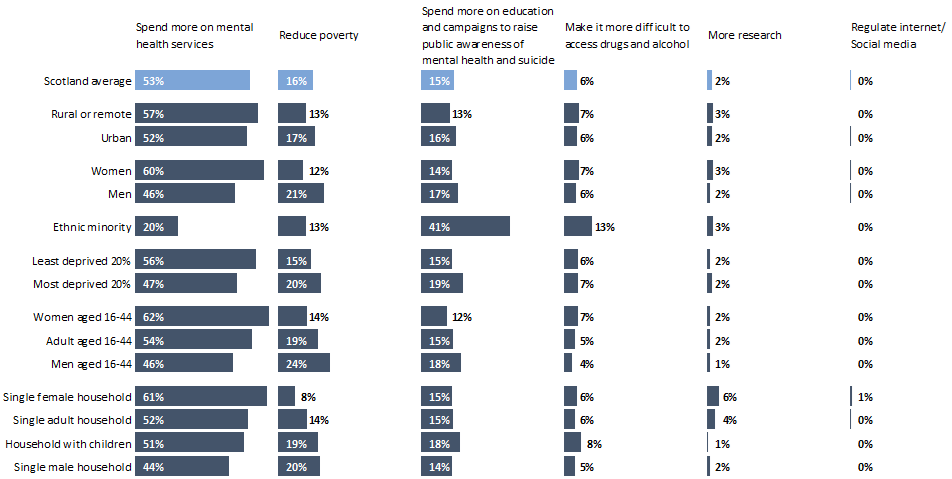
The Scottish Social Attitudes Survey also asked: “Which of the following, if any, do you think would be the most effective way of reducing deaths in Scotland from suicide?”
Unlike with deaths from drugs and alcohol, the data suggest people in Scotland overwhelmingly feel that an increase in spending on mental health services would be the most effective way of reducing deaths from suicide. Beyond this, preferences were similar to people’s views on the most effective ways of reducing deaths from drugs and alcohol.
As with drugs and alcohol, women were more likely to choose mental health service spending and less likely to choose poverty reduction compared to average, whilst men were the opposite.
There were similar differences between people who identified as White and people from minority ethnicities. 41% of people from ethnic minority backgrounds felt that spending more on education and campaigns to raise public awareness on mental health and suicide would be the most effective, compared to 15% if the population as a whole.
The fact that investing in mental health services was by far the most popular option may reflect wider public concern and advocacy pressure around access and long waiting times for accessing mental health support in Scotland (57).
The finding that people from ethnic minority backgrounds were much more likely than others to choose spending on more on education and awareness raising campaigns could reflect broader research which finds that people from minority ethnic communities in Scotland and the wider UK often experience more stigma around mental ill health, as well as experiencing discrimination when seeking support (58). Indeed, Scottish Government commissioned research has found that stigma can intersect with experiences of discrimination to create reluctance to seek mental health support among some racialised groups (59), which could also explain why people from minority ethnic backgrounds were so much less likely than other groups to choose investing in mental health services when answering this survey question.
Chart 9: Which of the following, if any, do you think would be the most effective way of reducing deaths in Scotland from suicide?
Fair treatment by public services
Broader survey evidence in Scotland suggests that most people report being treated with dignity and respect by public services, particularly in areas such as local health services (60). However, this positive picture is uneven: perceptions of fairness and service quality vary by service area, geography and social position, and concerns about declining standards and responsiveness, especially in core services such as health, have increased in recent years (61,62). A review of qualitative research in Scotland also identified multiple reports from people in more socially disadvantaged communities feeling that public services stigmatise, deprioritise and discriminate against them (14).
Evidence from labour market surveys and employment research suggests that a majority of workers in Scotland report generally positive experiences of workplace treatment and access to fair opportunities, particularly in workplaces with stronger employment practices such as trade union recognition, collective bargaining, and formal human-resources policies (63,64). However, this overall picture masks significant inequalities: a substantial minority of workers report unfair treatment, including discrimination, harassment and limited progression opportunities, with these experiences disproportionately concentrated among people in insecure or low-paid work, those with weaker workplace voice or representation, and groups protected under equality legislation such as disabled people, women and minority ethnic workers (65,66).
There is also recent survey evidence that finds that people from black and minority ethnic communities in Scotland report experience high levels of discrimination, across employment (40% when seeking jobs, 38% in career advancement), policing/criminal justice (34%), healthcare (30%), transport (27%), and education (25%). Compared to previous surveys undertaken by the same team, the latest round suggests that the confidence of Black and minority ethnic communities in anti-discrimination efforts in Scotland has declined over time (67).
Where people feel they have been treated poorly or unfairly, research consistently shows this is associated with lower trust in public institutions and reduced willingness to engage with services, reinforcing patterns of disengagement among people experiencing poverty, disability or other forms of disadvantage (62,68).
What the Scottish Social Attitudes Survey found
In this context, the Scottish Social Attitudes survey asked: “Over the past 12 months, do you feel that, on the whole, you have been treated fairly or unfairly when using public services, such as the health service, schools/colleges, or services provided by your local council?”
Most people in Scotland felt that they had been treated fairly, very fairly, or neutrally by public services. A small number of people (5%) said they had not used any public services in the last year.
People living in least deprived areas were the least likely to say they had experienced unfair treatment, while people from most deprived areas were the most likely to say they had experienced unfair treatment. Interestingly, people from minority ethnic backgrounds were the least likely to report feeling they had been treated unfairly in the services they have used in the past year.
Chart 10: Over the past 12 months, do you feel that, on the whole, you have been treated fairly or unfairly when using public services, such as the health service, schools/colleges, or services provided by your local council?
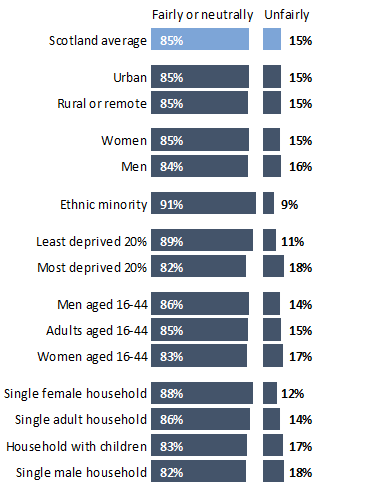
Note: This counts people who responded that they were or are treated “very fairly,” “fairly” “neither fairly nor unfairly,” “unfairly,” or “very unfairly.” This excludes respondents who “have not used public services in the last 12 months,” “don’t know,” or “prefer not to answer.”
The Scottish Social Attitudes Survey also asked: “In your last or current job, how fairly or unfairly do you feel you were/are treated by your employer?”
The results suggest that 81% of working-aged people in Scotland feel they have been treated fairly or neutrally at work, with 5% of people saying they hadn’t worked in a long time. Excluding the group who reported not having worked in a long time, around 15% of all working age people in Scotland felt that they had been treated unfairly in their last or current job.
Among working aged adults who had worked recently worked, women who live by themselves (and, similarly, women aged 16-44) were the most likely to cite unfair treatment at work, although gendered gaps for men and women more generally were negligible. People from minority ethnic communities were slightly less likely than the Scottish average to report feeling they had been treated unfairly by their employer. People living in rural or remote areas were the least likely to cite unfair treatment at work overall.
Chart 11: In your last or current job, how fairly or unfairly do you feel you were/are treated by your employer?
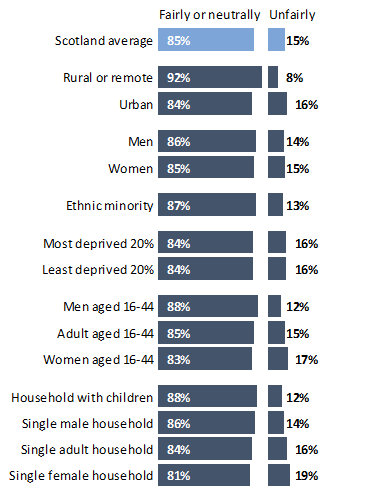
Note: This counts people aged 16-64 who responded that they were or are treated “very fairly,” “fairly” “neither fairly nor unfairly,” “unfairly,” or “very unfairly.” This excludes respondents who “have not been in work in a very long time,” “don’t know,” or “prefer not to answer.”
When we contrast the responses of people from the most and least deprived areas of Scotland for the two questions in this section, the results paint rather a mixed picture. The fact that people from the most deprived areas were more likely than people from the least deprived areas to report feeling that they had been treated unfairly by public services in the last year aligns with existing qualitative research in which more socially disadvantaged groups in Scotland report feeling uncared for and deprioritised (14). This result, surprisingly, does not carry over to employment, where both groups were similarly likely to report unfair treatment.
Likewise, the fact that people from minority ethnic communities were less likely than the Scottish average to report feeling they had been treated unfairly by public services and employers was unexpected in the context of recent survey research identifying widespread experiences of discrimination (67). There are three potential reasons for this apparent mismatch. First, where unfair treatment is chronic or normalised, people may adapt by discounting marginal events or treating them as “how it is” rather than as reportable injustice (69). Second, survey responses are affected not only by people’s experiences but by their willingness to disclose these experiences and previous research (67) suggests people from minority ethnic communities in Scotland may be wary of reporting discrimination and unfair treatment. Finally, there is some selection bias in our responses, in that we opted to exclude those who responded to this question by saying that they “haven’t worked in a very long time.” 19% of working-aged people from ethnic minority backgrounds chose this option, compared to 5% of people in Scotland as a whole.
Conclusion
This briefing provides timely evidence from the latest Scottish Social Attitudes survey on how people in Scotland understand health inequalities, their causes, and the role of government in addressing them.
Public concern about health inequalities is very high, with overwhelming agreement that government action to reduce the health gap between richer and poorer groups is important (94% of people said it was either quite or very important).
The survey also highlights widespread support for a greater focus on prevention, with most people favouring a balanced approach between preventative action and services. Achieving this balance would require a substantial shift towards prevention from the current policy mix. However, people living in the most deprived areas place greater emphasis on the continued importance of treatment and crisis support, reflecting lived experiences of acute need and inequality.
While many people initially identify individual behaviours such as smoking, alcohol use and diet as key drivers of health inequalities, responses across the survey demonstrate a broader understanding of the underlying social determinants of health. For example, deaths from drugs and alcohol are primarily seen as a social problem, with reducing poverty identified as the most effective response, and very limited support for punitive approaches. For suicide, investment in mental health services is the most strongly supported option, but poverty reduction was the second most popular choice.
There are marked differences in the views of people in the most and least deprived areas of Scotland across several questions: people living in more deprived areas are more likely to emphasise the role of stress, smoking and drinking, while those in less deprived areas more often highlight diet. The different views on smoking and drinking may reflect inequalities in the harms caused by alcohol and tobacco products (which fall more heavily on Scotland’s disadvantaged communities) and contrasting commercial landscapes (existing research demonstrates that tobacco, alcohol and fast food are concentrated in more disadvantaged urban areas). The different views on diet may speak to a disconnect between a policy concern with obesity and overweight and lived experience of food insecurity in Scotland’s more disadvantaged communities. More broadly, the contrasting views of those in Scotland’s least and most deprived areas underlines the markedly different experiences of those at the sharp end of inequalities.
Public preferences for addressing housing shortages, improving housing quality and supporting people into work are spread across multiple options, suggesting strong support for multi-faceted policy approaches rather than single solutions.
With Scottish Parliamentary elections due to take place in May 2026, these findings offer important insights for political parties, policymakers and civil society organisations. They suggest a strong public mandate for action to reduce health inequalities through tackling poverty and improving key social determinants, alongside progress towards a preventative shift in policy. At the same time, high pressures arising from crisis situations – such as the national housing emergency – and socially patterned experiences of unfair treatment mean there will continue to be expectations that reactive services remain adequately resourced and accessible.
Taken together, the evidence suggests that future policy agendas are likely to resonate most strongly with people in Scotland where they combine decisive action on poverty, housing and employment, support a sustained shift towards prevention, and demonstrate visible commitments to fairness, access and support for those currently experiencing the sharpest health inequalities. The current fiscal climate, in which there is pressure to reduce public spending (70), makes developing sustainable policy options across these areas particularly challenging.
Annex
Annex 1: Examined and reported variables
Variables that were used in this analysis:
Annex 2: Scottish Social Attitudes Survey Technical Details
Sample design
The SSA survey is designed to yield a representative sample of people aged 16 or over living in Scotland. Since 1999, the sampling frame for the survey has been the Postcode Address File (PAF), a list of addresses (or postal delivery points) compiled by the Post Office.
For practical reasons, the sample is confined to those living in private households. People living in institutions (though not in private households at such institutions) are excluded, as are households whose addresses were not on the PAF.
Selection of addresses and dwelling units/households
In 2025, a stratified sample of 15,078 unclustered addresses was drawn from the PAF across the whole of Scotland (12,565 for the main sample, and 2,513 for the reserve), including the Highlands and Islands.
Stratification enhances the efficiency of sample design by increasing precision, reducing variability, and ensuring representativeness by controlling for differences between subgroups. The method involves dividing the population into distinct subgroups, known as strata, based on specific characteristics relevant to the study. Each stratum is then sampled separately.
2025 Fieldwork
Sampled addresses were sent letters inviting up to two respondents per household to complete the survey.
While respondents were encouraged to complete the survey online, they were given the option of conducting the survey by telephone. This was to try to ensure that the offline population, and those who are less likely to take part online, still had the opportunity to take part.
Telephone interviews were conducted by interviewers from NatCen’s Telephone Unit. Before fieldwork, interviewers attended a briefing to familiarise themselves with the questionnaire and the study.
Fieldwork was carried out between 2nd September and 12th October 2025 for both modes.
Questionnaire
Each address was allocated at random to one of two versions of the questionnaire, each of which covered a different mixture of topics. All versions of the questionnaire collected key demographic information about participants.
Response rate
After taking into account the estimated number of eligible people aged 16 or over per sampled address and the estimated proportion of addresses that were deadwood or ineligible, the individual and household level response rates have been calculated as follows:
2,300 households (18% of all issued addresses) fully or partially completed at least one questionnaire. Information on non-responding addresses is not fully captured in push-to-web surveys, so it is not possible to record accurately the number of selected addresses which were not eligible because, for example, they are non-residential addresses. If we assume the level of such addresses is the same as in the 2019 SSA survey (10%), the estimated household response rate in 2025 was 20%. Given an assumed average of 1.9 eligible adults per address and a total of 3,043 productive interviews (fully and partially complete interviews), there was an individual response rate of 14.2%. Of the total productive interviews, 3,014 were completed via the web survey and 29 were telephone interviews.
[1] Estimate based on SSA 2019 % of ineligible
[2] The number of households with at least one response as a proportion of all issued addresses
[3] The number of households with at least one response as a proportion of all the eligible sample (i.e. adjusted for deadwood/ineligible)
Citation
Please use the following citation for referencing this report
Catalano, A., Smith, K. E., & Jack, D. (2026). Poverty, Prevention and Fairness: Public attitudes to health inequalities and the social determinants of health in the Scottish Social Attitudes Survey. Available at: https://doi.org/10.17868/strath.00095807
Acknowledgements
We are grateful to the Scottish Centre for Social Research for help with the development of the questionnaire and for collecting the data.
SHERU is supported by the Health Foundation, an independent charitable organisation working to build a healthier UK, as part of its Driving improving health and reducing inequalities in Scotland programme.
References
1. National Records of Scotland. Healthy Life Expectancy, 2021-2023 [Internet]. 2025 [cited 2026 Mar 2]. Available from: https://www.nrscotland.gov.uk/publications/healthy-life-expectancy-2021-2023/
2. Catalano A, Congreve E, Jack D, McHardy F, Smith K. 2025 Inequality Landscape : Health and Socioeconomic Inequality in Scotland in 2025 [Report] [Internet]. Glasgow: Scottish Health Equity Research Unit; 2025 Sep [cited 2026 Mar 2]. Report No. Available from: https://doi.org/10.17868/strath.00094201
3. Scottish Government. Long-term Monitoring of Health Inequalities March 2023 report [Internet]. 2023 [cited 2026 Mar 2]. Report No. Available from: https://www.gov.scot/publications/long-term-monitoring-health-inequalities-march-2023-report/
4. Warren S. Following, not leading: politicians and public opinion on action to support better health. The King’s Fund [Internet]. 2022 [cited 2026 Mar 2]. Available from: https://www.kingsfund.org.uk/insight-and-analysis/blogs/following-not-leading-politicians-public-opinion-support-better-health
5. Smith K. Beyond Evidence Based Policy in Public Health: The Interplay of Ideas. Springer; 2013. 269 p.
6. McHugh N, Baker R, Bambra C. Policy actors’ perceptions of public participation to tackle health inequalities in Scotland: a paradox? Int J Equity Health. 2023 Mar 30;22(1):57. doi:10.1186/s12939-023-01869-8
7. McGarrol S. Contextualising lifestyles: how socially contrasting places in Fife, Scotland influence lay understandings of lifestyle and health behaviours in relation to coronary heart disease. Health Place. 2020 Nov 1;66:102432. doi:10.1016/j.healthplace.2020.102432
8. Popay J, Bennett S, Thomas C, Williams G, Gatrell A, Bostock L. Beyond ‘beer, fags, egg and chips’? Exploring lay understandings of social inequalities in health. Sociol Health Illn. 2003;25(1):1–23. doi:10.1111/1467-9566.t01-1-00322
9. Bolam B, Murphy S, Gleeson K. Individualisation and inequalities in health: a qualitative study of class identity and health. Soc Sci Med. 2004 Oct 1;59(7):1355–65. doi:10.1016/j.socscimed.2004.01.018
10. McNulty C, Sides E, Thomas A, Kamal A, Syeda RB, Kaissi A, et al. Public views of and reactions to the COVID-19 pandemic in England: a qualitative study with diverse ethnicities. BMJ Open. 2022 Aug 1;12(8):e061027. doi:10.1136/bmjopen-2022-061027 PubMed PMID: 35977758.
11. Kane M, Thornton J, Bibby J. Building public understanding of health and health inequalities [Internet]. 2022 [cited 2026 Mar 2]. Available from: https://www.health.org.uk/reports-and-analysis/briefings/building-public-understanding-of-health-and-health-inequalities
12. The Diffley Partnership. Health Inequalities in Scotland: Public Engagement Research. 2022. Report No.
13. Blaxter M. Whose fault is it? People’s own conceptions of the reasons for health inequalities. Soc Sci Med. 1997 Mar 1;Health Inequalities in Modern Societies and Beyond44(6):747–56. doi:10.1016/S0277-9536(96)00192-X
14. Smith K, Stewart E. Under attack? Public accounts of health inequalities and the social determinants of health in Scotland. J Crit Public Health. 2024 May 20;1(2):5–23. doi:10.55016/ojs/jcph.v1i2.77753
15. Smith KE, Anderson R. Understanding lay perspectives on socioeconomic health inequalities in Britain: a meta-ethnography. Sociol Health Illn. 2018;40(1):146–70. doi:10.1111/1467-9566.12629
16. Garthwaite K, Bambra C. “How the other half live”: Lay perspectives on health inequalities in an age of austerity. Soc Sci Med. 2017 Aug 1;187:268–75. doi:10.1016/j.socscimed.2017.05.021
17. ASH Scotland. Smoking and health inequalities in Scotland [Internet]. 2024 [cited 2026 Mar 2]. Available from: https://ashscotland.org.uk/wp-content/uploads/2024/07/Smoking-and-Health-Inequalities_April-2024.pdf
18. Public Health Scotland. Alcohol consumption and harms dashboard: update briefing. 2025. Report No.
19. Scottish Government. The Scottish Health Survey 2023 – volume 1: main report [Internet]. 2024 [cited 2026 Mar 2]. Report No. Available from: https://www.gov.scot/publications/scottish-health-survey-2023-volume-1-main-report/pages/11/
20. Obesity Action Scotland. Obesity in Scotland: Prevalence, Causes, Impact and Responses [Internet]. 2025 [cited 2026 Mar 2]. Available from: https://www.obesityactionscotland.org/media/sw5ome13/obesity-in-scotland-prevalence-causes-impact-and-responses-march-2025.pdf
21. Macdonald L, Olsen JR, Shortt NK, Ellaway A. Do ‘environmental bads’ such as alcohol, fast food, tobacco, and gambling outlets cluster and co-locate in more deprived areas in Glasgow City, Scotland? Health Place. 2018 May 1;51:224–31. doi:10.1016/j.healthplace.2018.04.008
22. Caryl F, Shortt NK, Pearce J, Reid G, Mitchell R. Socioeconomic inequalities in children’s exposure to tobacco retailing based on individual-level GPS data in Scotland. Tob Control. 2020 Jul 1;29(4):367–73. doi:10.1136/tobaccocontrol-2018-054891 PubMed PMID: 31278083.
23. Shortt NK, Tisch C, Pearce J, Mitchell R, Richardson EA, Hill S, et al. A cross-sectional analysis of the relationship between tobacco and alcohol outlet density and neighbourhood deprivation. BMC Public Health. 2015 Oct 5;15(1):1014. doi:10.1186/s12889-015-2321-1
24. McNamara S, Holmes J, Stevely AK, Tsuchiya A. How averse are the UK general public to inequalities in health between socioeconomic groups? A systematic review. Eur J Health Econ HEPAC Health Econ Prev Care. 2020 Mar;21(2):275–85. doi:10.1007/s10198-019-01126-2 PubMed PMID: 31650439; PubMed Central PMCID: PMC7072057.
25. Smith KE, Macintyre AK, Weakley S, Hill SE, Escobar O, Fergie G. Public understandings of potential policy responses to health inequalities: Evidence from a UK national survey and citizens’ juries in three UK cities. Soc Sci Med. 2021 Dec 1;291:114458. doi:10.1016/j.socscimed.2021.114458
26. Scottish Government. Christie Commission on the future delivery of public services [Internet]. 2011 [cited 2026 Mar 2]. Available from: https://www.gov.scot/publications/commission-future-delivery-public-services/
27. Public Health Scotland. Public Health Scotland’s strategic plan 2022 to 2025 [Internet]. 2025 [cited 2026 Mar 2]. Available from: https://publichealthscotland.scot/about-us/what-we-do-and-how-we-work/a-scotland-where-everybody-thrives-public-health-scotland-s-strategic-plan-2022-to-2025/
28. Scottish Government. Scotland’s Population Health Framework [Internet]. 2025 [cited 2026 Mar 2]. Available from: https://www.gov.scot/publications/scotlands-population-health-framework/
29. Congreve E, McHardy F, Smith K. Raising the roof [Internet]. 2025 [cited 2026 Mar 2]. Available from: https://scothealthequity.org/wp-content/uploads/2025/09/housingreport-organized.pdf
30. SHERU. Prevention Watch October 2024. Scottish Health Equity Research Unit [Internet]. 2024 Oct 17. Available from: https://scothealthequity.org/prevention-watch-october-2024/
31. Ipsos. Public perceptions of health and social care May 2023 (Wave 4) [Internet]. 2023 [cited 2026 Mar 2]. Available from: https://www.health.org.uk/sites/default/files/2025-04/Public%20perceptions%20of%20health%20and%20social%20care%20May%202023%20%28Wave%204%29.pdf
32. Audit Scotland. Alcohol and drug services. 2024.
33. Bogie J, Dijk M van, Bezzina C, Lunan C, Henderson D, Mercer SW, et al. Addressing the inverse care law in Scottish general practice: systematic scoping review. Br J Gen Pract. 2025 Aug 1;75(757):e549–58. doi:10.3399/BJGP.2024.0622 PubMed PMID: 40355249.
34. Independent Healthcare Provider Network. People in higher social grades are more likely to have used private healthcare [Internet]. 2023 [cited 2026 Mar 2]. Available from: https://www.ihpn.org.uk/people-in-higher-social-grades-are-more-likely-to-have-used-private-healthcare/
35. Scottish Housing News. Crisis: One in four Scots directly affected by homelessness [Internet]. 2025. Available from: https://www.scottishhousingnews.com/articles/crisis-one-in-four-scots-directly-affected-by-homelessness
36. Public Health Scotland. Homelessness and Health Inequalities [Internet]. 2026 [cited 2026 Mar 2]. Available from: https://publichealthscotland.scot/population-health/social-and-economic-impacts-on-health/equity-and-justice/homelessness/homelessness-and-health-inequalities
37. Jack D. Collaborative Research for Meaningful Impact. Scottish Health Equity Research Unit [Internet]. 2025 May 28 [cited 2026 Mar 4]. Available from: https://scothealthequity.org/collaborative-research-for-meaningful-impact/
38. Gibson M, Petticrew M, Bambra C, Sowden AJ, Wright KE, Whitehead M. Housing and health inequalities: a synthesis of systematic reviews of interventions aimed at different pathways linking housing and health. Health Place. 2011 Jan;17(1):175–84. doi:10.1016/j.healthplace.2010.09.011 PubMed PMID: 21159542; PubMed Central PMCID: PMC3098470.
39. Hergenrather K, Zeglin R, McGuire-Kuletz M, Rhodes S. Employment as a Social Determinant of Health: A Systematic Review of Longitudinal Studies Exploring the Relationship Between Employment Status and Physical Health. Rehabil Res. 2015 Feb 1;29. doi:10.1891/2168-6653.29.1.2
40. Eiser D, Congreve E, Crummey C, Catalano A. Health Inequalities in Scotland [Internet]. 2022 [cited 2026 Mar 2]. Available from: https://fraserofallander.org/wp-content/uploads/2022/11/FAI-Health-Foundation-Final-Report-2.pdf
41. Awan-Scully R. Public Attitudes to Social Housing in Scotland. 2020.
42. Zemanik M. Working Lives Scotland 2023 [Internet]. 2023 [cited 2026 Mar 2]. Available from: https://www.cipd.org/globalassets/media/knowledge/knowledge-hub/reports/2023-pdfs/2023-working-lives-scotland-report-8407-final.pdf
43. Scottish Government. Economic inactivity in Scotland: supporting those with longer-term health conditions and disabilities to remain economically active [Internet]. 2024 [cited 2026 Mar 2]. Available from: https://www.gov.scot/publications/economic-inactivity-scotland-supporting-those-longer-term-health-conditions-disabilities-remain-economically-active/
44. Scottish Government. Households in Scotland by housing tenure: Scottish Household Survey, 2023 [Internet]. 2024 [cited 2026 Mar 2]. Available from: https://www.gov.scot/publications/households-in-scotland-by-housing-tenure-scottish-household-survey-2023/
45. Ryder DB. Still waiting for a home: Stories of people waiting for social housing. 2025.
46. National Records of Scotland. Drug-related deaths in Scotland, 2024 [Internet]. 2025 [cited 2026 Mar 2]. Available from: https://www.nrscotland.gov.uk/publications/drug-related-deaths-in-scotland-2024/
47. Office for National Statistics. Alcohol-specific deaths in the UK [Internet]. 2025 [cited 2026 Mar 2]. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/causesofdeath/bulletins/alcoholrelateddeathsintheunitedkingdom/registeredin2023
48. Garratt K, Kirk-Wade E, Gajjar D, Danechi S. Suicide prevention policy [Internet]. 2026 Mar 2 [cited 2026 Mar 2]. Available from: https://commonslibrary.parliament.uk/research-briefings/cbp-10090/
49. Royal College of Psychiatrists. www.rcpsych.ac.uk [Internet]. 2024 [cited 2026 Mar 2]. Drug and drink deaths in Scotland still among Europe’s worst despite new funding. Available from: https://www.rcpsych.ac.uk/news-and-features/latest-news/detail/2024/10/31/drug-and-drink-deaths-in-scotland-still-among-europe-s-worst-despite-new-funding
50. Turkmen A. Later Life Accounts of Drug Use in the UK. University of Strathclyde. Report No.
51. Richardson C, Dickson A, Robb KA, O’Connor RC. The Male Experience of Suicide Attempts and Recovery: An Interpretative Phenomenological Analysis. Int J Environ Res Public Health. 2021 Jan;18(10):5209. doi:10.3390/ijerph18105209
52. Chandler A. Masculinities and suicide: unsettling ‘talk’ as a response to suicide in men. Crit Public Health. 2021;32(4):499–508. doi:https://doi.org/10.1080/09581596.2021.1908959
53. Scottish Government. Creating Hope Together: suicide prevention action plan 2022 to 2025 [Internet]. 2022 [cited 2026 Mar 2]. Available from: https://www.gov.scot/publications/creating-hope-together-scotlands-suicide-prevention-action-plan-2022-2025/
54. Scottish Government. Preventing Harm, Promoting Recovery: Scotland’s Alcohol & Drugs Strategic Plan 2026 – 2035 [Internet]. 2026 [cited 2026 Mar 18]. Available from: https://www.gov.scot/publications/preventing-harm-promoting-recovery-scotlands-alcohol-drugs-strategic-plan-2026-2035/
55. Diffley Partnership. Commercial Determinants of Health and Public Attitudes: A Deliberative Research Approach [Internet]. 2023 [cited 2026 Mar 2]. Available from: https://diffleypartnership.co.uk/wp-content/uploads/2024/05/NCD-Deliberative-Research-Diffley-Report.pdf
56. Thompson S. Poverty among young adult men in Scotland. Scottish Health Equity Research Unit [Internet]. 2026 Feb 12 [cited 2026 Mar 2]. Available from: https://scothealthequity.org/poverty-among-young-adult-men-in-scotland/
57. SAMH. Scottish Government Mental Health Strategy Consultation – SAMH Response [Internet]. 2022 [cited 2026 Mar 2]. Available from: https://www.samh.org.uk/documents/Scottish_Government_Mental_Health_Strategy_SAMH_submission_-_Sept_2022.pdf
58. Alam S, O’Halloran S, Fowke A. What are the barriers to mental health support for racially-minoritised people within the UK? A systematic review and thematic synthesis. Cogn Behav Ther. 2024 Jan;17:e10. doi:10.1017/S1754470X24000084
59. Jackson I, Wasige J, Moody RK, Opeloyeru O, Masinde I, Wasige C. Experiences of Adversely Racialised People In Scotland Related to Suicide Ideation. Scottish Government; 2021. Report No.
60. Scottish Government. Scottish Household Survey 2024: Satisfaction with Local Health Services and Sport and Leisure Facilities [Internet]. 2025 [cited 2026 Mar 2]. Available from: https://www.gov.scot/publications/scottish-household-survey-2024-local-health-services-and-local-authority-sport-and-leisure-facilities/
61. Scottish Government. Scottish Social Attitudes Survey 2023 – Attitudes to Government, the Economy, and the Health Service [Internet]. 2024 [cited 2026 Mar 2]. Available from: https://www.gov.scot/publications/scottish-social-attitudes-survey-2023-attitudes-government-economy-health-service/
62. Scottish Government. Scottish Household Survey 2023: trust in public institutions [Internet]. 2024 [cited 2026 Mar 2]. Available from: https://www.gov.scot/publications/scottish-household-survey-2023-trust-public-institutions/
63. Scottish Government. Fair Work: action plan [Internet]. 2019 [cited 2026 Mar 2]. Available from: https://www.gov.scot/publications/fair-work-action-plan/
64. Bryson A, Forth J, Gray H, Stokes L. Does Employing Older Workers Affect Workplace Performance? Ind Relat J Econ Soc. 2020;59(4):532–62. doi:10.1111/irel.12265
65. Scottish Government. Discrimination and Harassment in Scotland, results from the 2023 Scottish Household Survey [Internet]. 2024 [cited 2026 Mar 2]. Available from: https://www.gov.scot/publications/discrimination-and-harassment-in-scotland-results-from-the-2023-scottish-household-survey/
66. Equality and Human Rights Commission. Is Scotland Fairer? [Internet]. 2018 [cited 2026 Mar 2]. Available from: https://www.equalityhumanrights.com/sites/default/files/is-britain-fairer-2018-is-scotland-fairer_0.pdf
67. Glasgow Social Sciences Hub. A survey shows racial discrimination is on the rise in Scotland [Internet]. 2025 [cited 2026 Mar 2]. Available from: https://www.gla.ac.uk/explore/glasgowsocialscienceshub/resources/all/headline_1157664_en.html
68. Poverty and Inequality Commission. Dignity and respect in public services: the view of people with direct lived experience of poverty [Internet]. 2020 [cited 2026 Mar 2]. Available from: https://povertyinequality.scot/wp-content/uploads/2020/02/Short-report-dignity-and-respect-in-public-services.pdf?utm_source=chatgpt.com
69. Major B, Quinton WJ, McCoy SK. Antecedents and consequences of attributions to discrimination: Theoretical and empirical advances. In: Advances in experimental social psychology, Vol. 34. San Diego, CA, US: Academic Press; 2002. p. 251–330. doi:10.1016/S0065-2601(02)80007-7
70. Scottish Fiscal Commission. Budget and Spending Review underscore tight fiscal outlook as Scottish Government plans efficiencies and reform [Internet]. 2026 Jan 13 [cited 2026 Mar 3]. Available from: https://fiscalcommission.scot/budget-and-spending-review-underscore-tight-fiscal-outlook-as-scottish-government-plans-efficiencies-and-reform/